登陆查看更多优秀资源帖,与同道便捷交流讨论
您需要 登录 才可以下载或查看,没有帐号?立即注册
x
Abstract
Among epilepsy-associated non-neoplastic lesions, mesial temporal lobe epilepsy with hippocampal sclerosis (mTLE-HS) and malformation of cortical development (MCD) including focal cortical dysplasia (FCD), are the two most frequent causes of drug-resistant focal epilepsies constituting about 50% of all surgical pathology of epilepsy. Several distinct histological patterns have been historically recognized in both HS and FCD, and several studies have tried to perform clinicopathological correlation; results, however, have been controversial, particularly in terms of postsurgical seizure outcome. Recently, the International League Against Epilepsy constituted a Task Forces of Neuropathology and FCD within the Commission on Diagnostic Methods, to establish an international consensus of histological classification of HS and FCD, respectively, based on agreement with the recognition of the importance of defining a histopathological classification system that reliably has some clinicopathological correlation. Such consensus classifications are likely to facilitate future clinicopathological study. Meanwhile, we reviewed neuropathology of 41 surgical cases of mTLE, and confirmed three type/patterns of HS along with no HS, based on the qualitative evaluation of the distribution and severity of neuronal loss and gliosis within hippocampal formation; i.e., HS type 1 (61%) equivalent to 'classical' Ammon's horn sclerosis, HS type 2 (2%) representing CA1 sclerosis, HS type 3 (17%) equivalent to end folium sclerosis, and no HS (19%)。 Furthermore we performed a neuropathological comparative study on mTLE-HS and dementia associated HS (d-HS) in elderly, and confirmed that neuropathological features differ between mTLE-HS and d-HS in the distribution of hippocampal neuronal loss and gliosis, morphology of reactive astrocytes and their protein expression, and presence of concomitant neurodegenerative changes particularly Alzheimer type and TDP-43 pathologies. These differences may account, at least in part, for the difference in pathogenesis and epileptogenicity of HS in mTLE and senile dementia. However, the etiology and pathogenesis of most epileptogenic lesions are yet to be elucidated.
INTRODUCTION
Over the last couple of decades, there has been an increasing opportunity to evaluate surgical pathology of drug-resistant focal epilepsy, owing largely to the development of sophisticated neuroimaging technologies including magnetic resonance image (MRI) and positron emission tomography (PET)。 Epilepsy, even though limited to patients with surgical indication, may be the consequence of a wide range of disorders affecting the brain including tumors and various non-neoplastic lesions.1–4 In fact, a broad spectrum of structural brain lesions have been confirmed by a survey of 5,392 epileptogenic brain tissue specimens surgically resected from patients with drug-resistant localized epilepsies collected at the European Epilepsy Brain Bank.5 These, in descending order of frequency, include hippocampal sclerosis (HS) (33.7%), long-term epilepsy-associated tumors (LEAT) (25.1%), malformations of cortical development (MCDs) (15.5%), vascular malformations (5.7%), dual pathologies (5.2%), glial scars (4.9%) and encephalitis (1.6%) as well as no lesion (8%)。 Besides LEAT, HS and MCDs are the two most frequent non-neoplastic lesions of drug-resistant focal epilepsies constituting about 50% of all epilepsy surgery cases. In this review article, neuropathological features of these two lesions will be briefly summarized, addressing the several distinct histological patterns that have historically been identified and classified in HS and focal cortical dysplasia (FCD)。 Furthermore, our recent attempt to construct a simplified classification system of HS based on the review of 41 surgical cases of mTLE, and neuropathological comparative study of mTLE-HS and dementia associated HS (d-HS) in the elderly will also be addressed. Finally, HS occurs not infrequently with a second lesion, including FCD. Current ILAE definitions of such combined HS and FCD will also be briefly summarized.
HIPPOCAMPAL SCLEROSIS
Hippocampal sclerosis (HS) is the most frequent pathologic finding in én bloc resection specimens from patients, usually in their twenties and thirties or occasionally even forties, with long-standing pharmacoresistant mesial temporal lobe epilepsy (mTLE)。 The earliest pathological study of epilepsy dates back to the early 19th century. Bouchet and Cazauvielh in 1825 described macroscopic features of hard and shrunken hippocampus in autopsy brains from patients with an antemortem history of epilepsy.6 Sommer in 1880 first described microscopic features of HS in an autopsy brain from a patient with mTLE.7 He observed loss of pyramidal neurons in a portion of the hippocampus that was later on called “Sommer's sector” corresponding to the sector CA1 of Lorente de Nó。8 Sommer also noted some neuronal loss within the hilus of the dentate gyrus. In 1899, Bratz performed histological investigation using autopsy cases with chronic epilepsy and described detailed histological features of unilaterally atrophic hippocampus, illustrating severe loss of pyramidal neurons and gliosis in Sommer's sector of the Ammon's horn, less severe neuronal loss in the hilus of the dentate gyrus and adjacent sector CA3, and preservation of neurons in the CA2, subiculum and the granule cell layer of the dentate gyrus.9 Of note, his illustration also clearly demonstrates a sharp boundary between lesioned CA1 sector and well-preserved subiculum to be oblique, which represents subicular-CA1 border zone or “prosubiculum” of Lorente de Nó。8 In fact, his description represents the most common and characteristic histological feature of HS. In 1966, Margerison and Corsellis defined two types of hippocampal damage.10 One was a pattern previously characterized by Bratz's description and termed 'classical' Ammon's horn sclerosis. Another pattern of hippocampal damage that they described was characterized by neuronal loss confined to the hilus of the dentate gyrus or 'end folium‘, termed 'end folium sclerosis (EFS)’。 In addition to those two patterns of HS, Bruton added, in his monograph published in 1988, a third pattern of HS called 'total' Ammon's horn sclerosis, showing almost complete neuronal loss in all sectors of the hippocampus.11 These specific patterns of HS could easily be assessed based solely on qualitative observation; however, Bruton found no apparent correlation between any of those specific types of HS and the clinical history among 107 patients in his study.
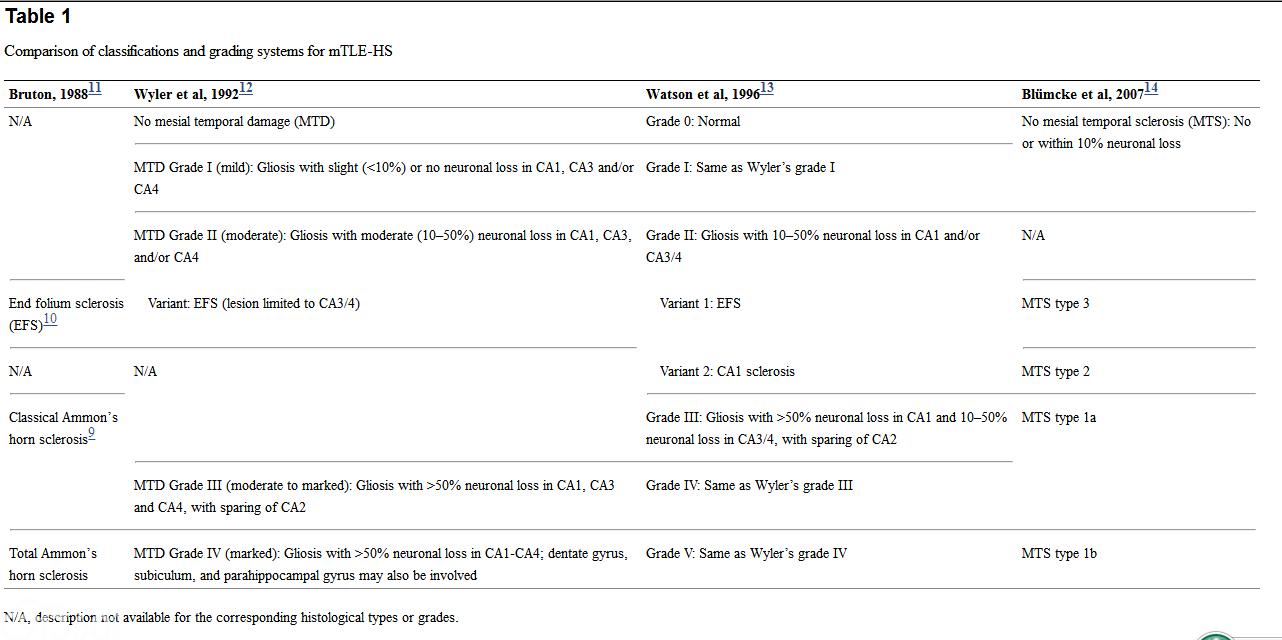
Since then, several proposals for classification and a grading system for HS have been published (Table 1)。 The first systematic attempt to semi-quantitatively evaluate the severity of hippocampal neuronal loss for the histological grading of HS was proposed by Wyler et al in 1992, providing four grades for HS along with a diagnosis of no HS introducing the term 'mesial temporal damage (MTD‘。12 Wyler's grading system revealed that classical and total Ammon's horn sclerosis were the most frequent pathologies in mTLE. Inverse clinicopathological correlation has been reported between Wyler's grade and postsurgical memory impairment; patients having the most postoperative memory loss were the ones with normal or grade I pathology, whereas those patients with high grades (III and IV) pathology showed little in terms of significant postoperative memory problems.13 Mossy fiber sprouting in the dentate gyrus as demonstrated by Timm's staining can be observed in cases with Wyler's high-grade lesions.14 In terms of memory impairment, histological patterns of granule cell pathology in the dentate gyrus have been reported to be associated with learning dysfunction in addition to older age at epilepsy surgery and longer duration of illness.15 A more recent study has demonstrated that the in vitro capacity of proliferation and differentiation into neurons of neural stem cells isolated from the dentate gyrus in patients with pharmacoresistant mTLE was significantly associated with preoperative memory performance and the number of granule cells in the resected specimen.16 Another study has shown that the younger age at seizure onset was associated with Wyler's high-grade pathology.17 In 1996, Watson et al proposed a six-tiered grading system that is a modification of Wyler's grading system, mainly by inserting an additional grade between Wyler's grades II and III.18
In 2007, Blümcke et al proposed a clinicopathological classification system for HS, using the term 'mesial temporal sclerosis (MTS)' based on the cluster analysis of semi-quantitative measurements of neuronal loss in CA1-CA4, showing five distinct patterns of hippocampal pathology.19 They found that these patterns were associated with specific clinical histories and/or postsurgical outcome; e.g., the age of the initial precipitating injury (IPI) appeared to be an important predictor of hippocampal pathology, as it was younger in patients with MTS types 1a and 1b (< 3 years) than those with MTS types 2 (mean 6 years) and 3 (mean 13 years) as well as no MTS (mean 16 years)。 While successful seizure control was associated with MTS types 1a and 1b, MTS type 3 (EFS) appears to be a predictor of poorer postsurgical seizure outcome. By contrast, Thom et al found better outcomes for patients with EFS and poorer outcomes for no HS group.20 Such differences in the results among various studies appear to be a major problem in elucidating the clinicopathological correlation of mTLE-HS, and seem to be associated, at least in part, with differences in the number of patients studied, inclusion and exclusion criteria and the surgical procedure employed, as well as postsurgical follow-up periods. Interobserver reliability would also affect the histological diagnosis and results of each individual study.
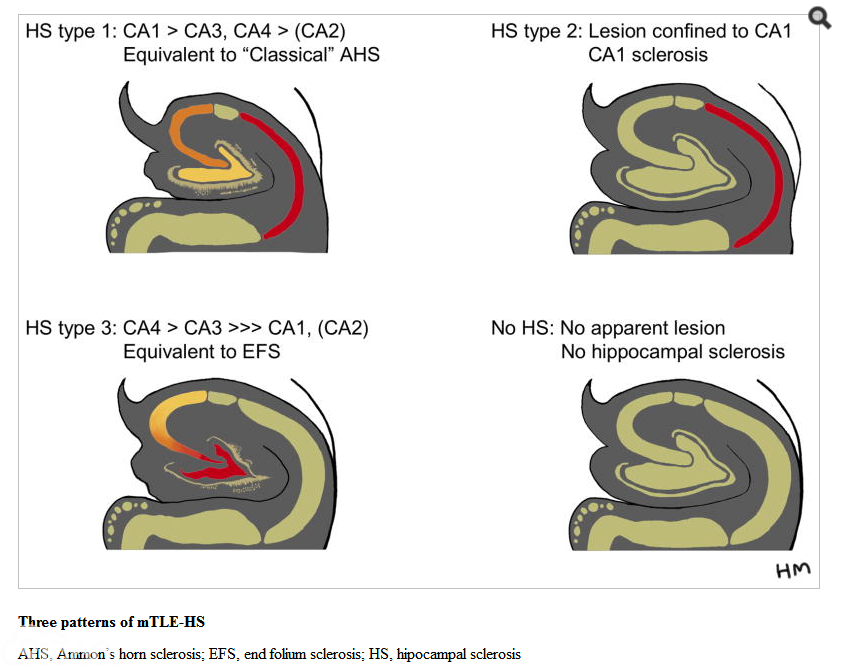
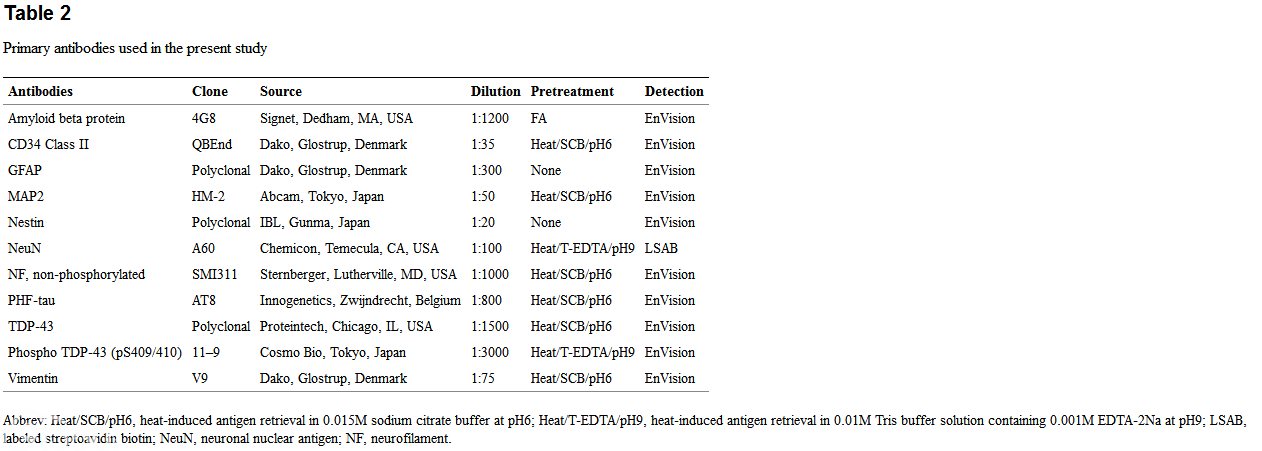
Recently, the International League Against Epilepsy (ILAE) constituted a task force of neuropathology within the Commission on Diagnostic Methods, trying to establish an international consensus of histological classification of HS using a semi-quantitative scoring system, based on agreement with the recognition of the importance of defining a histopathological classification system that reliably has some clinicopathological correlation such as postsurgical seizure outcome and memory impairment.21 A new classification will be proposed in the near future. Meanwhile, the authors (HM and TH) reviewed surgical specimens obtained from consecutive 41 mTLE patients (male/female=24/17; age at onset, 14.7±11.7 years old; age at operation, 32.8±10.8 years old; postoperative follow-up period, 27–253 months) treated by selective amygdalohippocampectomy with or without temporal lobectomy between 1991 and 2010, excluding 7 cases due to insufficient amount of tissue available for histological study. All patients were operated on by one of the authors (TH) in Tottori University, Tokyo Women's Medical University, and Moriyama Memorial Hospital, Japan. Histological evaluation was performed on formalin-fixed, paraffin-embedded tissue sections stained by HE and Klüver-Barrera as well as a panel of immunohistochemistry for GFAP, vimentin, and NeuN (Table 2)。 Based on the neuropathological findings of our 41 cases, together with the Blümcke's classification,19 we tried to classify hippocampal pathology based on the qualitative evaluation of the distribution and severity of neuronal loss and gliosis within hippocampal formation, and recognized three types/lesion patterns of HS (Figure 1); i.e., HS type 1 (25 of 41 cases, 61%) is equivalent to 'classical' Ammon's horn sclerosis9 in which neuronal loss and gliosis is the most severe in CA1, followed by CA3, CA4, with relative sparing of CA2 and often associated with loss of dentate granule cells and/or dispersion. HS type 2 represents neuronal loss and gliosis almost confined to CA1 (CA1 sclerosis), and only 1 case (2%) was identified in our study. HS type 3 (7 cases, 17%) is characterized by a reverse distribution of the sclerotic lesion to HS type 1, in which neuronal loss and gliosis is the most severe in CA4 followed by CA3, with relative sparing of CA2 and CA1, that is equivalent to EFS.10 In addition to these three HS types, we also identified 8 cases (19%) without apparent neuronal loss and gliosis (no HS)。 Subiculum was relatively well-preserved in all cases. Our study also confirmed HS type 1 to be the most frequent pathology in mTLE. Strictly speaking, precise borders between each hippocampal subfields/sectors (CA1~4) and CA1/prosubiculum border are not determinable without Golgi staining in specimens form healthy individuals,8 and each border is still unclear even in specimens from patients with mTLE showing segmental neuronal loss. However, since recognition of the distribution and severity of neuronal loss (lesion patterns) by visual inspection of KB stained and/or NeuN immunostained sections (Figure 2) seems easy and practical for many pathologists to assess histological changes and make diagnoses, clinicopathological correlation study based on such a qualitative and simplified histological classification will also be waranted.
Fig. 1
Fig. 2
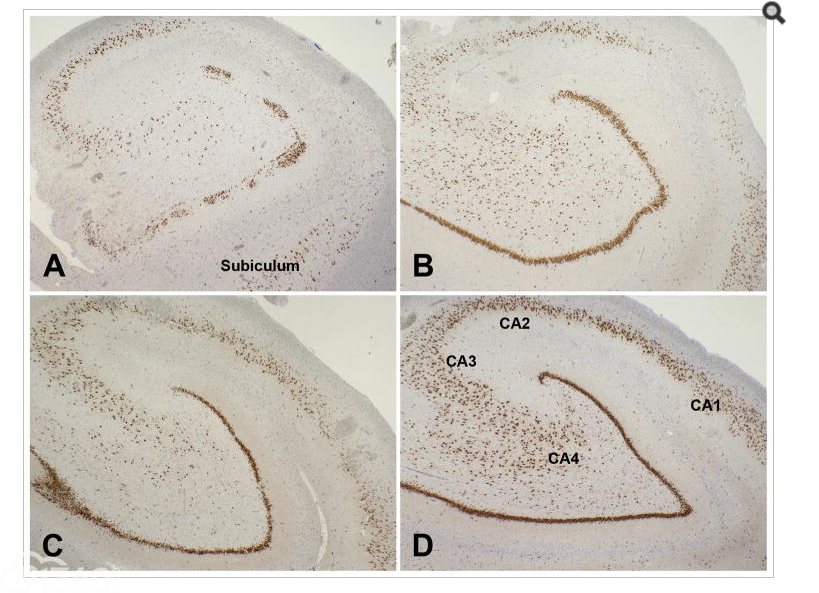
Representative findings of NeuN immunohistochemistry of surgically resected hippocampi from patients with mTLE
A: HS type 1 showing neuronal loss, almost complete in CA1, moderate to marked in CA4, and mild in CA3, with relative sparing of CA2 and subiculum. Dentate granule cell layer shows both neuronal loss and dispersion.
B: HS type 2 showing neuronal loss in CA1 with relative sparing of other sectors.
C: HS type 3 showing marked neuronal loss in CA4 with sparing of other sectors.
D: No Hs showing well preserved hippocampal neurons.
NeuN immunohistochemistry counterstained with hematoxylin.
“HIPPOCAMPAL SCLEROSIS” IN EPILEPSY VERSUS SENILE DEMENTIA
The term 'hippocampal sclerosis' has been used for the neuropathological substrate not only for mTLE but also for dementia in the elderly clinically characterized by severe amnesia and slowly progressive dementia without clinical seizure activity, that is difficult to distinguish clinically from Alzheimer's disese.22,23 In this review article, the authors use the term 'dementia with hippocampal sclerosis (d-HS)' after the term 'mTLE-HS' for 'mesial temporal lobe epilepsy with hippocampal sclerosis’。 Histological feature of d-HS may be observed in a given autopsy brain without significant other pathology (2–4%), but it is frequently found in combination with other dementing illness including vascular and neurodegenerative disorders (12–20% of cases)。24 Among 382 autopsy cases with dementia from the State of Florida Brain Bank, d-HS constituted 13%, and 66% of d-HS cases had concomitant Alzheimer's disease.25 To clarify the difference between mTLE-HS and d-HS, the authors (HM and HVV) have performed histological and immunohistochemical comparative study on hippocampi and amygdalae obtained from 7 autopsy cases of dementia (6 archival cases from UCLA Alzheimer's Disease Research Center and 1 case from Research Institute for Brain and Blood Vessels - Akita) and those obtained from above mentioned 41 surgical cases of mTLE including 41 hippocampi and 36 amygdalae available for study.26 Formalin-fixed paraffin-embedded specimens were cut at 5 μm thickness, subjected to HE and KB staining as routine procedures. Adjacent serial sections were subjected to immunohistochemistry for a panel of primary antibodies shown in Table 2. Deparaffinized sections were subjected to antigen retrieval procedure if needed before incubation with 3% H2O2 diluted in distilled water for 30 min followed by appropriate blocking solutions. Sections were incubated with primary antibodies overnight at 4°C, followed by incubation with goat anti-rabbit immunoglobulins conjugated to peroxidase labeled-dextran polymer (EnVision System-HRP, Dako, Carpinteria, CA, USA) for 45 min at 37°C. For NeuN immunostaining, streptoavidin-biotin-peroxidase complex method was employed. Immunoreaction was visualized by 3–3'diaminobenzidine tetrahydrochloride (DAB, Dako, Carpinteria, CA, USA)。 Sections were counterstained with hematoxylin. Immunostaining with omission of primary antibodies was used as a negative control.
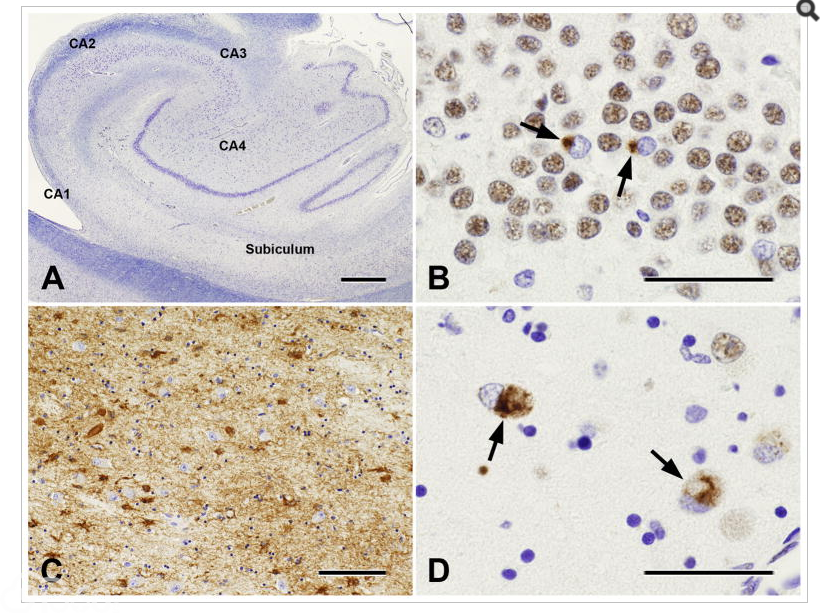
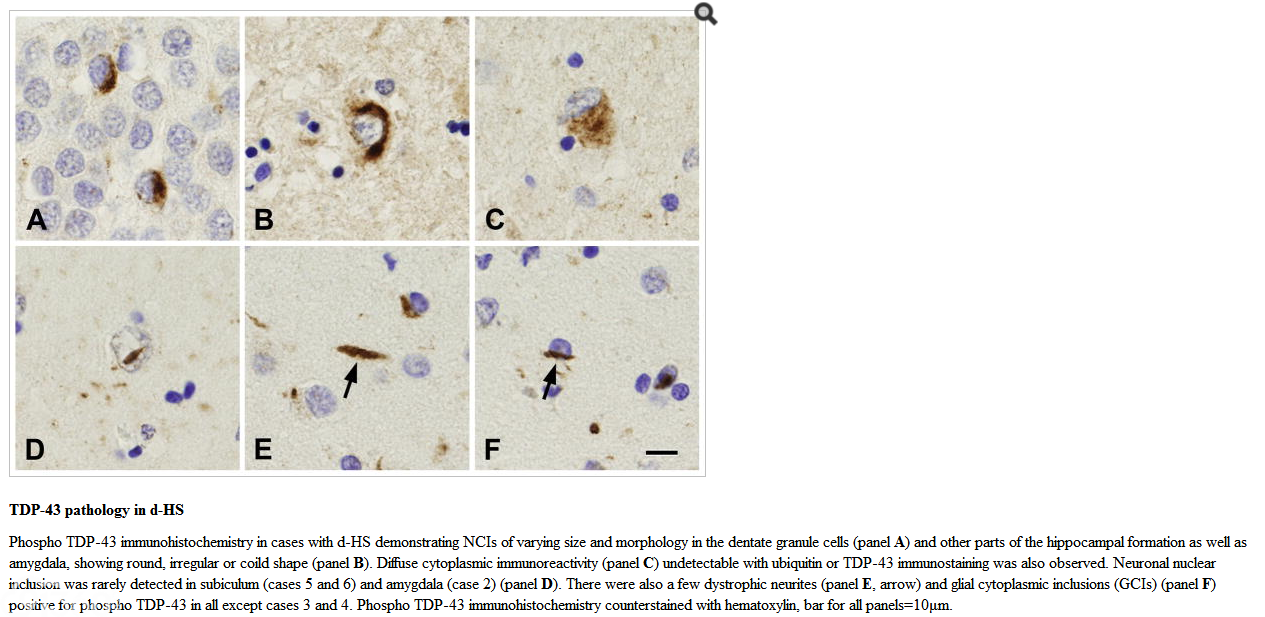
In all d-HS autopsy cases, neurons in CA1-subiculum were constantly depleted and other sectors and dentate gyrus were relatively well preserved. In one case (case 7), severe neuronal loss and gliosis were also observed in all other sectors of the hippocampus and the dentate gyrus in addition to the lesion in CA1-subiculum. Lesion was found unilaterally (on the left side) in 4 cases and bilaterally in 3 cases. Reactive astrocytes had eosinophilic plump cytoplasm and processes that were immunoreactive for GFAP but not vimentin. Six of 7 cases had severe Alzheimer type pathology27,28 (neurofibrillary tangles and senile plaques of both diffuse and neuritic-types) with or without cerebral amyloid angiopathy of varying severity,29 and concomitant TDP-43 proteinopathy (Table 3)。 One case (case 6) had frontotemporal lobar degeneration with TDP-43 pathology. TDP-43 pathology was observed in all cases except case 3 and characterized by scattered neuronal cytoplasmic inclusions (NCIs) that are immunoreactive for ubiquitin, TDP-43 and phospho TDP-43, along with loss of normal nuclear labelling with TDP-43 in the granule cell layer of the dentate gyrus, and TDP-43/phospho TDP-43 immunoreactive NCIs of larger size in the remaining neurons with a small number of TDP-43-positive putative dystrophic neurites and glial cytoplasmic inclusions (GCIs) in the regions of CA1, subiculum and parahippocampal cortex as well as amygdala (Figure 3)。 TDP-43-positive neuronal nuclear inclusions (NNIs) were rarely detected in the subiculum or amygdala in 3 of 7 cases. Phospho TDP-43 immunohistochemistry specifically detected many more NCIs, NNIs, dystrophic neurites and GCIs as well as abnormal neurons showing diffuse cytoplasmic staining of phospho TDP-43 that were not detected by ubiquitin and TDP-43 immunostainings (Figure 4)。
Fig. 3
Hippocampus and amygdala from an autopsy brain of a 91-year-old man (case 5) with neuropathologically comfirmed Alzheimer's disease and bilateral hippocampal sclerosis
A: Severe neuronal loss is noted in CA1 and subiculum, with relative sparing of other sectors of the hippocampus and dentate granule cells. Klüver-Barrera method, bar=500μm.
B: TDP-43 immunoreactive neuronal cytoplasmic inclusions (NCIs) in the dentate granule cells with loss of nuclear immunoreactivity (arrows)。 TDP-43 immunohistochemistry counterstained with hematoxylin, bar=50μm.
C: Marked gliosis is evident in the amygdala, although the number of neurons appears relatively well-preserved. Note each reactive astrocyte has GFAP-positive plump cytoplasm and fine processes. GFAP immunohistochemistry counterstained with hematoxylin, bar=50μm.
D: TDP-43 immunoreactive NCIs are observed in the amygdala, more pronounced in the corticomedial rather than basolateral nuclear group. A few TDP-43 positive neurites were also observed in another area (data not shown)。 TDP-43 immunohistochemistry counterstained with hematoxylin, bar=50μm.
Fig. 4
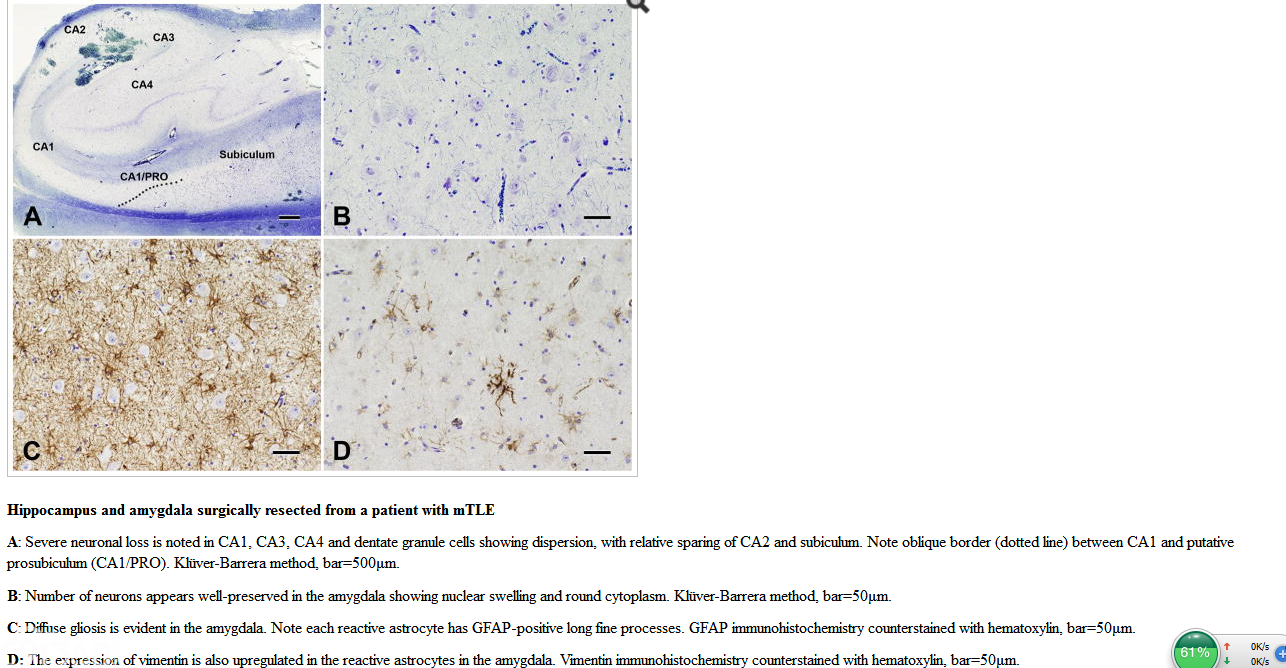
By contrast, in mTLE cases, three different patterns of neuronal loss and gliosis were recognized in mTLE-HS along with no HS as mentioned above, without known neurodegenerative conditions including tauopathy and TDP-43 proteinopathy, and subiculum was well preserved in all cases. Neurons in the amygdala showed nuclear swelling and round cytoplasm in 23 of 36 (63.9%) cases. No significant neuronal loss was observed in the amygdala (except in one case) regardless of the presence or absence of HS, but abundant reactive astrocytes having fine processes with cytoplasmic upregulation of GFAP and vimentin were noted in 31 of 36 (86.1%) cases (Figure 5), suggesting a possible functional significance of astrocytes in the amygdala in the epileptogenesis of mTLE.
Fig. 5
These results clearly indicate that neuropathological features differ between mTLE-HS and d-HS in the distribution of hippocampal neuronal loss and gliosis, morphology of reactive astrocytes and their protein expression, and presence or absence of concomitant neurodegenerative changes. Furthermore, these differences may account, at least in part, for the difference in pathogenesis and epileptogenicity of HS in mTLE and senile dementia.
FOCAL CORTICAL DYSPLASIA
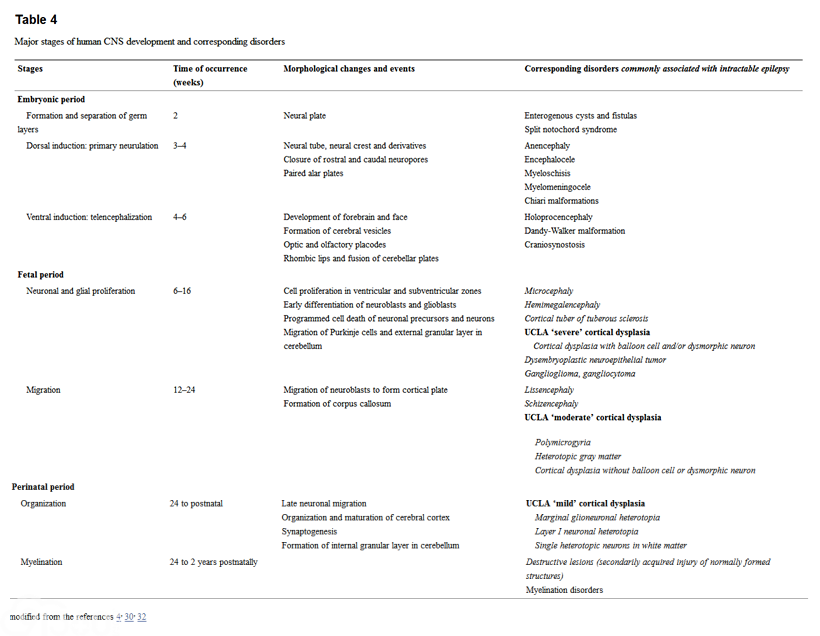
Development of the human cerebral neocortex
The neuropathologic changes seen in patients, particularly children, with epilepsy frequently represent the end results of insults to a developing brain. Cerebral neocortical development after neural tube formation is considered to be the result of a series of overlapping processes: (a) cell proliferation in the ventricular and subventricular zones (VZ/SVZ), (b) early differentiation of neuroblasts and glioblasts, (c) programmed cell death of neuronal precursors and neurons, (d) migration of neuroblasts to form the cortical plate, (e) late neuronal migration, (f) organization and maturation of cortex, and (g) synaptogenesis.4,30,31,32 A growing number of genetic and molecular mechanisms has been identified and shown to be associated with abnormalities of these processes that may result in abnormalities of cortical architecture and presumably its electrophysiological properties.33 Most developmental disorders of the brain commonly associated with epilepsy are thought to originate from the perturbations of each developmental event after the embryonic period; i.e., after 6 weeks' gestation when cell proliferation starts along the wall of the neural tube to generate a collection of 'matrix cell'34 or precursor cells for all neuroblasts and glioblasts, forming VZ/SVZ in the pallium, as well as ganglionic eminence in the subpallium (Table 4)。 The neuronal component in the cerebral neocortex consists of glutamatergic excitatory (70–80%) and GABAergic inhibitory (20–30%) neurons. Neuroblasts of the former are generated in the pallial VZ/SVZ and migrate along the processes of radial glia to reach the cortical plate (radial migration) which is formed in an “inside-out” fashion, as neuroblasts born first destined for the deepest cortical layers migrate first, while neuroblasts born later destined for the more superficial cortical layers migrate past the already settled cortical neuroblasts,35 eventually forming a six-layered structure.36 Radial glial cells have long been known to serve as guides for the migrating neuroblasts and finally produce cortical astrocytes. However, recent evidence in rodents indicates that radial glial cells are multipotent progenitor cells, generating projection neurons in the developing cerebral cortex37–39 and a subpopulation of oligodendrocytes.40,41 Studies using human fetal brain also indicate that radial glia are neuronal42 and oligodendrocyte43 progenitor cells. Abnormalities of radial glia may occur with various molecular mechanisms either focally or diffusely in malformations of cortical development (MCDs), including Fukuyama congenital muscular dystrophy (FCMD)44 and tuberous sclerosis complex (TSC)。45 Neuroblasts of the GABAergic inhibitory neurons, on the other hand, are generated in the ganglionic eminence near the basal ganglia and migrate tangentially to the pial surface (tangential migration) to enter the cortical plate.46,47 Perturbation of the generation of those interneurons is responsible for lissencephaly.
Focal cortical dysplasia (FCD): histological features and classifications
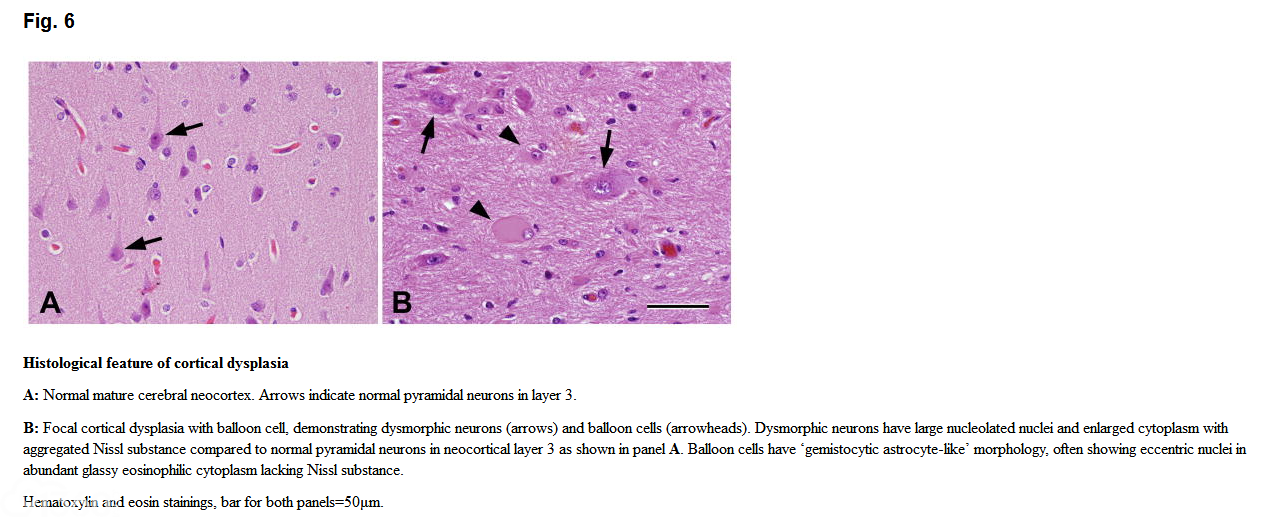
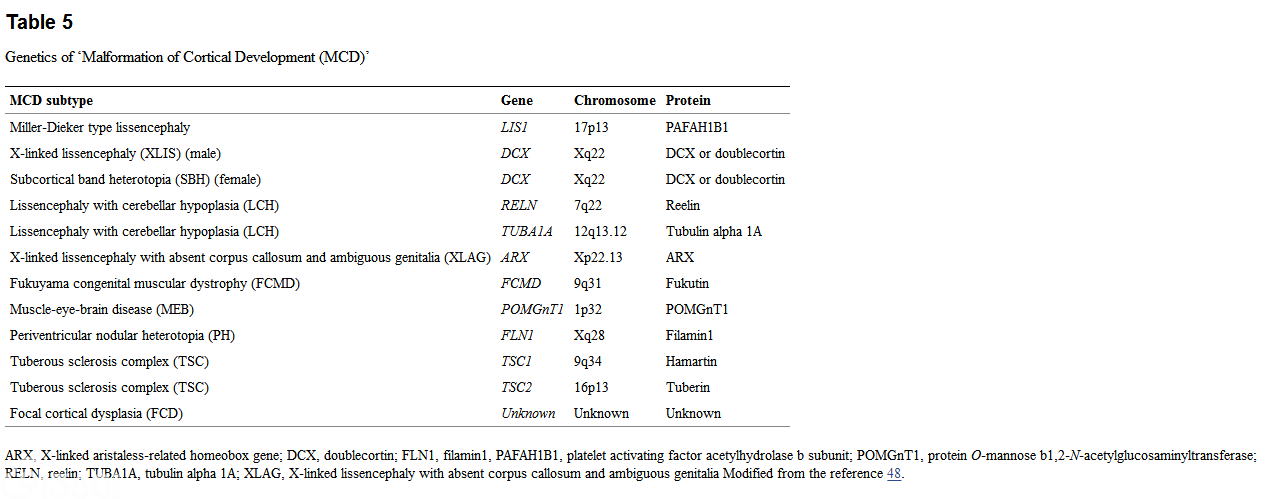
MCD consists of a heterogeneous group of disorders, in which the normal hexalaminar structure of the cerebral neocortex is disrupted (architectural abnormality) and individual neuronal morphologies may be aberrant (cytoarchitectural abnormality)。 Several genes responsible for epilepsy-associated MCDs have been identified over the past two decades (Table 5),33,48 and the functions of those genes have been intensively studied mostly in transgenic or knockout mice, allowing for better understanding of the molecular pathomechanism of each disorders.48 Focal cortical dysplasia (FCD) of Taylor type (T-FCD),49 a subset of MCDs, has been known to be strongly associated with infantile spasms and medically intractable epilepsy in young children, accounting for 20% of epilepsy patients in some previous reports.50,51 Surgical resection of epileptogenic lesions has evolved as an efficient strategy in the treatment of patients with T-FCD.52,53 The lesion is histologically characterized by cortical laminar disorganization and the presence of dysmorphic neurons with/without characteristic large gemistocytic astrocyte-like “balloon cell (BC)”, and has been classified in some recent proposals as 'severe' FCD in the ULCA classification54, FCD type IIA (without BC) / IIB (with BC) in Palmini's classification55 or FCD type IIa (without BC) / IIb (with BC) in ILAE classification.56 These histological features are very similar to those seen in cortical tubers of tuberous sclerosis complex (TSC-tubers) (Figure 6),48,57 despite different clinical presentations. Recent evidence has suggested factors significant in the morphogenesis of abnormal cells in dysplastic cortex of TSC-tubers and FCD type IIb, including aberrant expression of cytoskeletal proteins,58,59 stem cell markers such as nestin,60 CD34 class II,61 neurotrophin receptors62, fibroblast growth factor-263,64 and cortical layer markers65 as well as altered mTOR signaling pathways.66,67 Some of these studies, at least from the neuropathological point of view, provided supportive evidence that BCs and dysmorphic neurons represent disturbed gliogenesis from matrix cells or radial glia and disturbed maturation of cortical neurons from migrating neuroblasts or intermediate progenitor cells, respectively. These results may also support the 'dysmature developmental hypothesis' that epileptogenesis in FCD type II is the consequence of local interactions of dysmature cells having immature cellular and synaptic properties with normal postnatal neurons.68
The presence of dysplastic oligodendroglial cells has also been suggested in MCDs with BC (TSC-tubers and FCD type IIb)。63 Based mainly on the similarities in morphological features and imunohistochemical profiles as well as altered mTOR signaling pathways between TSC-tubers and FCD type II, these two lesions are presumed to be 'cortical dysgenesis with abnormal cell proliferation but without neoplasia' in early stages of the developing brain.33 However, cellular and molecular as well as genetic mechanisms underlying the pathogenesis of FCD type II are largely unknown.
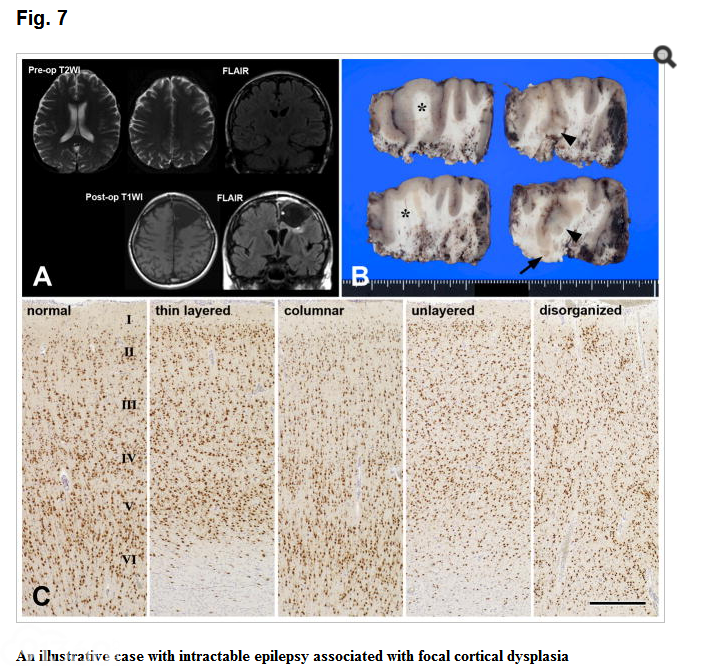
Currently, FCD is a heterogeneous group of disorders commonly associated with medically intractable epilepsy mainly in children. The cellular pathology of FCD can be stratified depending on whether or not certain specific microscopic abnormalities are noted in a given specimen. Mischel et al54 reviewed over 70 examples of cortical dysplasia from young patients who underwent hemispherectomy or lobectomy, and the following eight major histopathologic features were scored as being present or absent in each specimen; 1) cortical laminar disorganization (a defining feature of cortical dysplasia and hence present in all specimens) (Figure 7), 2) single heterotopic neurons within the deep white matter or molecular layer (layer I) of cortex (94.4%), 3) neuronal cytomegaly (63.9%), 4) neuronal cytoskeletal abnormalities69 (55.6%), 5) macroscopically visible neuronal heterotopias, usually in the subcortical white matter (40.3%), 6) foci of polymicrogyria (PMG) (13.9%), 7) neuroglial excrescences in the subarachnoid space (13.9%), and 8) balloon cells (18.1%)。 Based on the presence or absence of various combinations of these histologic features, individual cases were subclassified as being mild, moderate, or severe in the first proposed grading system (Table 4)54. Preliminary correlation of the severity of cortical dysplasia with clinical severity of the seizure disorder has shown that mean preoperative seizure frequency correlated well with the histologic grade, and children with moderate or severe degrees of cortical dysplasia were more likely to have shown a preoperative neurologic deficit. Another study on cortical dysplasia cases in the UCLA pediatric and adult epilepsy surgery cohort (n=97) determined nine histopathologic elements including 1) cortical disorganization and dyslamination as an essential feature of cortical dysplasia, 2) excessive heterotopic white matter neurons (99%), 3) dysmorphic-cytomegalic neurons (52%), 4) balloon cells (40%), 5) excessive heterotopic neurons in cortical molecular layer (40%), 6) marginal and nodular glioneuronal heterotopia (30%), 7) polymicrogyria (27%), 8) immature neurons (15%), and 9) persistence of subpial or superficial granular cell layer (8%)。70 Histogram of the frequency of patients with increasing histopathologic elements showed that most patients with cortical dysplasia had two to five (median: 3) features of abnormal cortical development among these nine histopathologic elements. Furthermore, most patients with Palmini type I cortical dysplasia had two histopathologic elements (median: 2), whereas patients with Palmini type II cortical dysplasia had a larger number of specific histological abnormalities (median: 4)。 Clinicopathological correlation revealed that patients with Palmini type II cortical dysplasia presented at younger ages, had higher seizure frequencies, and were more likely to have multilobar and hemispheric cortical dysplasia that involved extratemporal cortical regions, compared with Palmini type I cortical dysplasia which was found more often in adult patients in the temporal lobe. There was no significant difference in the postsurgical seizure outcome between patients with Palmini type I and type II cortical dysplasia in UCLA cohort70 and in other epilepsy center.71 However, some studies reported less favorable outcome in patients with Palmini type I cortical dysplasia,72,73 and other studies reported opposite results,74 although a significant proportion of these patients also had HS. Such inconsistent results among various studies also appear to be a major problem in elucidating the clinicopathological correlation of cortical dysplasia as being discussed in HS, and may be due, at least in part, to the difference in inclusion and exclusion criteria.
A 26-year-old Japanese woman clinically diagnosed as cingulate seizure since the age 19, presenting with simple and complex partial seizures, automatism, palpitation and hyperventilation. MRI (panel A) showed T2 high signal change in the left superior and middle frontal subcortical white matter. FDG-PET demonstrated hypometabolism in the left anterior cingulate gyrus. Under the preoperative diagnosis suggestive of focal cortical dysplasia, the patient underwent surgical intervention. Cut sections of the én bloc resection specimen after fixation showed focal blurring of cortex-white matter junction and uneven cortical thickness (e.g., asterisks in panel B) as well as abnormal gyral pattern (e.g., arrowheads in panel B)。 Cluster of subcortical nodular heterotopias were also noted (arrow in panel B)。 Neu N immunohistochemistry (panel C) revealed various patterns of focal abnormal neuronal arrangement and layering in the cerebral cortex, including imcompletely layered with reduced thickeness, predominant vertical columnar structure with equivocal cortex-white matter junction, unlayered and disorganized neuronal arrangements. Compare relativey normal hexalaminar structure of normal cortical thickensss (left in panel C)。 Based on the presence of both abnormal radial and tangential cortical laminations, together with scattered hypertrophic neurons outside layer 5, but no dysmorphic neuron or balloon cell, neuropathological diagnosis of FCD type Ic was made in this case. The patient is seizure free for more than 2 years after the operation (Engel class I)。 Bar in panel C=500μm.
Recently a consensus histological classification scheme of FCD was proposed at the initiative of the Task Force on FCD in the ILAE Diagnostic Methods Commission.56 The major changes from Palmini's classification to the ILAE classification included separation of 'isolated' FCD type I from those associated with other epileptogenic principal lesions; i.e., HS, tumors, vascular malformations, and any other lesion acquired during early life such as trauma, ischemic injury and encephalitis, and classifying these 'associated' counterparts as FCD type III, forming a three-tiered classification system (Table 6)。 Histological definition of FCD type I was reorganized in the ILAE classification. Another change was also made in the terminology; the term 'giant neurons' in Palmini's classification is now designated as 'hypertrophic neurons' in the ILAE classification, that is defined as large pyramidal neurons resembling those of neocortical layer 5 abnormally located in layers 1, 2, 3 or 4. Hypertrophic neurons can be observed in all types of FCD. Of note, the term 'giant cells' refers to large gemistocytic astrocyte-like cells observed in TSC-tubers, that are morphologically identical to 'balloon cells' observed in FCD type IIb. Although the etiology and pathogenesis of each FCD type are yet to be elucidated, this new classification seems applicable in terms of good interobserver and intraobserver agreement75 to the future clinicopathological correlation study for evaluating postsurgical seizure outcome in patients with 'isolated' FCD types I and II without any other epileptogenic lesions. One study using ILAE classification demonstrated poorer postsurgical outcome in patients with FCD type III than in patients with isolated FCD (FCD types I and II)。76
COMBINED HIPPOCAMPAL SCLEROSIS AND FOCAL CORTICAL DYSPLASIA
HS occurs not infrequently with a second lesion including FCD, either in the temporal or extratemporal lobe, mostly ipsilateral to the HS. Such a coexistent second lesion can be the epileptogenic principal lesion (dual pathology) or a potentially/questionably epileptogenic mild/subtle cortical developmental abnormality (FCD type IIIa)。 ILAE FCD classification proposes definitions of these two terminologies.
1. Dual pathology
Dual pathology is defined as HS with a coexistent second principal lesion affecting the brain, including tumor, vascular malformation, glial scar, limbic/Rasmussen encephalitis, and MCD (including FCD type II but not FCD type I)。 Of note, two independent epileptogenic principal lesions, but not including HS, affecting one or multiple lobes in a given patient is defined as “double pathology”。
2. FCD type IIIa
Architectural abnormalities (histologically equivalent to FCD type I) in the temporal lobe associated with HS are classified as FCD type IIIa, but not “dual pathology”, in the current ILAE FCD classification. Temporal cortex may show architectural abnormality (cortical dyslamination) or cytoarchitectural abnormalities (hypertrophic neurons outside layer 5) in patients with HS. The following five patterns can be recognized as FCD type IIIa variants:
HS with architectural abnormalities in the temporal lobe
HS with temporal lobe sclerosis (TLS)77
HS with TLS and heterotopic neurons in subcortical white matter
HS with TLS and small “lentiform” heterotopias in subcortical white matter
HS with small “lentiform” heterotopias in subcortical white matter
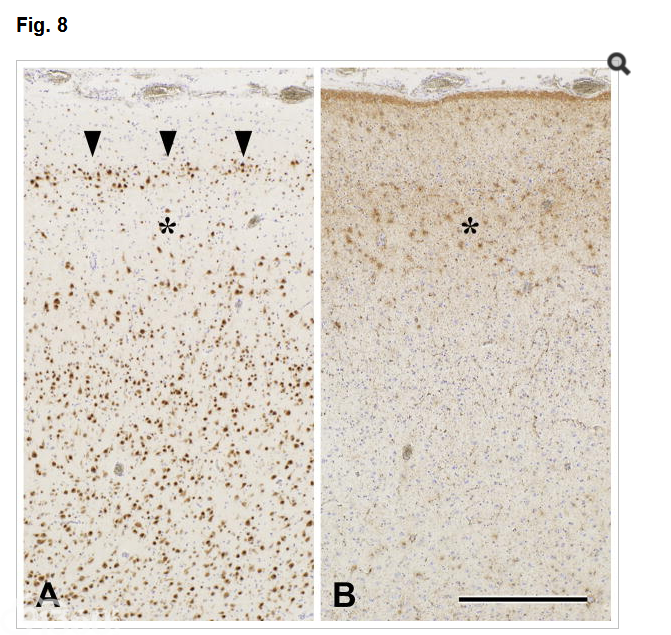
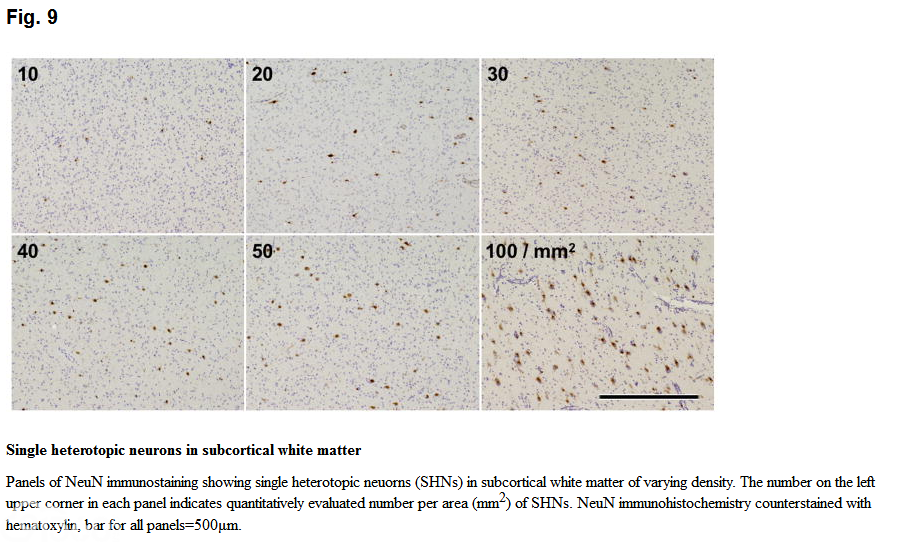
TLS is thought to represent severe neuronal loss and laminar gliosis in cortical layers 2 and 3, and cortical reorganization as suggested by the presence of horizontal bundles of aberrant myelinated fibers in this area. Actually, TLS can be observed in about 10% of surgical cases of mTLE as an abnormal band of small and clustered “granular” neurons in the outer part of cortical layer 2 (Figure 8)。77 Single heterotopic neurons in subcortical white matter should be considered significant when their number in deep white matter is more than 30/mm2,55 although their epileptogenic significance remains to be determined. For practical purposes, a panel of NeuN immunostaining may be useful to estimate the number of single heterotopic neurons in deep white matter (Figure 9); however, reference photographs should be prepared by each laboratory as the actual magnification of photographs differs depending on the microscope and attached digital camera as well as the distance between the optical lens and digital camera. Finally, small “lentiform” heterotopia is usually undetectable by MRI and histologically composed of projecting neurons, which is distinct from the larger nodular heterotopia that is usually detectable by MRI and consists of both projecting and local circuit neurons.78 Because of the similarity at a glance, it should not be mistaken for a part of the claustrum.
Temporal lobe sclerosis observed in a 43-year-old man with mTLE since the age 24
Pre-operative MRI showed T2/FLAIR high intensity change in the right atrophic hippocampus. FDG-PET revealed hypometabolism in the right temporal tip to mesial temporal structure. The patient underwent surgical intervention by combined amygdalohippocampectomy and anterior temporal lobectomy on the right side. Pathological examination of the resection specimen revealed hippocampal sclerosis (HS) with granule cell loss in the dentate gyrus and amygdala sclerosis as well as a feature of temporal lobe sclerosis (TLS) in the temporal neocortex shown in panels A and B. Based on the presence of TLS in association with HS, cortical abnormality in this case is consistent with one variant of FCD type IIIa. The patient is seizure free for more than 2 years after the operation (Engel class I)。
A: An abnormal band of small and clustered “granular” neurons in the outer part of cortical layer 2 (arrowheads) and underlying paucicellular area (asterisk)。 NeuN immunohistochemistry counterstained with hematoxylin.
B: Laminar gliosis in cortical layers 2 and 3 (asterisk), corresponding to the paucicellular area showin in panel A. GFAP immunohistochemistry counterstained with hematoxylin.
Bar for both panels=500μm.
CONCLUSION
Surgical pathology of mTLE-HS and FCD was briefly reviewed with some historical notes on their histological classifications and clinicopatholgical correlations, along with our recent attempts to construct a simplified classification system of HS and neuropathological comparative study on mTLE-HS and d-HS. However, the etiology and pathogenesis of most epileptogenic lesions, including mTLE-HS and FCD, are yet to be elucidated.
【本站为非盈利学术交流平台,部分资料来源于网络,如涉及版权问题请及时联系管理员处理;所有文章仅供公益交流,不代表本站立场。欢迎提供素材、资料等,投稿邮箱:tougao@91360.com,一经采纳将给予稿费。】
|






 发表于 2017-12-20 18:30:53
发表于 2017-12-20 18:30:53