登陆查看更多优秀资源帖,与同道便捷交流讨论
您需要 登录 才可以下载或查看,没有帐号?立即注册
x
Abstract
An accurate and complete pathology report is critical for the optimal management of cutaneous melanoma patients. Protocols for the pathologic reporting of melanoma have been independently developed by the Royal College of Pathologists of Australasia (RCPA), Royal College of Pathologists (United Kingdom) (RCPath), and College of American Pathologists (CAP). In this study, data sets, checklists, and structured reporting protocols for pathologic examination and reporting of cutaneous melanoma were analyzed by an international panel of melanoma pathologists and clinicians with the aim of developing a common, internationally agreed upon, evidence-based data set. The International Collaboration on Cancer Reporting cutaneous melanoma expert review panel analyzed the existing RCPA, RCPath, and CAP data sets to develop a protocol containing “required” (mandatory/core) and “recommended” (nonmandatory/noncore) elements. Required elements were defined as those that had agreed evidentiary support at National Health and Medical Research Council level III-2 level of evidence or above and that were unanimously agreed upon by the review panel to be essential for the clinical management, staging, or assessment of the prognosis of melanoma or fundamental for pathologic diagnosis. Recommended elements were those considered to be clinically important and recommended for good practice but with lesser degrees of supportive evidence. Sixteen core/required data elements for cutaneous melanoma pathology reports were defined (with an additional 4 core/required elements for specimens received with lymph nodes). Eighteen additional data elements with a lesser level of evidentiary support were included in the recommended data set. Consensus response values (permitted responses) were formulated for each data item. Development and agreement of this evidence-based protocol at an international level was accomplished in a timely and efficient manner, and the processes described herein may facilitate the development of protocols for other tumor types. Widespread utilization of an internationally agreed upon, structured pathology data set for melanoma will lead not only to improved patient management but is a prerequisite for research and for international benchmarking in health care.
Melanoma is a major public health problem in many countries, particularly those with a large population of fair-skinned individuals. Melanoma is the third most common cancer in both men and women in Australia, the fifth in both men and women in the United States, and the 12th in men and sixth in women in the United Kingdom.1 Furthermore, in many Western countries, both incidence and mortality rates are increasing. Because melanoma is one of the commonest cancers in young adults, it has a disproportionate effect on those in the most productive years of life.1 Nevertheless, accurate diagnosis and appropriate treatment at an early clinical stage are associated with high cure rates.2
Pathologic assessment of a tissue biopsy is a critical aspect in the multidisciplinary management of melanoma patients. Histologic parameters of the primary tumor are the strongest predictors of outcome in patients with clinically localized primary melanoma and strongly influence the next stages of management. Accordingly, accurate assessment and documentation of important pathologic variables are essential. Of even greater importance is the need to accurately determine whether a cutaneous melanocytic lesion is benign or malignant (ie, nevus or melanoma).3 For this reason, pathology reports of melanocytic lesions should: (1) document the key diagnostic criteria on which the diagnosis was based; and (2) provide histologic and other parameters important for patient prognosis and treatment.4 Documentation of the microscopic features is important not only for clinical governance but also to indicate the process of diagnostic decision-making and describe any areas of uncertainty.
In recent years, there has been widespread recognition of the need to improve the quality and completeness of cancer pathology reports to improve patient care. As part of this endeavor, pathology organizations have published recommended pathology data sets and reporting protocols for various cancers, including melanoma.5–9 Structured reporting aims to improve the completeness and usefulness of pathology reports for clinicians and improve the decision-making process for cancer treatment. The structured reporting protocol provides a framework for the assessment and documentation of all the pathologic features of any given case. Consistency and speed of reporting is improved by the use of discrete data elements recorded from the checklist.5,6 However, pathologists are encouraged to include free text or narrative to document any other relevant issues, to give reasons for coming to a particular opinion, and to explain any points of uncertainty. The evidence for prognostic markers may change over time, and a structured reporting template must therefore be updated regularly to be of maximal value.
Although pathology data sets for each cancer have been developed independently by various organizations, they have involved interpretation of virtually the same evidence. As a consequence, there is much commonality between the various data sets for individual cancers with minor differences reflecting differences in local practices or in interpretation. The current study was performed to harmonize the Royal College of Pathologists (United Kingdom) (RCPath), College of American Pathologists (CAP), and Royal College of Pathologists of Australasia (RCPA) data sets, checklists, and structured reporting protocols for cutaneous melanoma,7–9 with the aim of producing a common, internationally agreed upon, evidence-based data set for melanoma pathology reporting.
METHODS
Recognizing that there was much commonality in purpose and duplication of effort in the development of separate cancer pathology reporting, in 2011 a round table meeting of representatives of the RCPA, RCPath, CAP, and the Canadian Association of Pathologists was held to form the International Collaboration on Cancer Reporting (ICCR). The stated goal was to produce evidence-based generic cancer data sets that could be used in each of the representative bodies' jurisdictions to replace existing protocols and to establish processes that could be utilized for developing all future organ-specific cancer data sets/protocols. As a pilot project, it was decided that agreed upon cancer data sets would be developed for the pathology reporting of melanoma, prostate carcinoma, lung carcinoma, and endometrial carcinoma.10,11 Each of the respective 4 organizations chose an ICCR “Pathology Lead” representative who was given overall responsibility for guiding the development of 1 of the 4 cancer protocols (D.W.E. for melanoma). For each cancer, the “Pathology Lead” nominated an expert review panel, comprising 2 specialists from each country. The “Pathology Lead” selected a chairperson for each panel to coordinate the development of the protocol. For melanoma, the panel comprised the following individuals: R.A.S. (Chair, pathologist, RCPA representative), D.W.E. (ICCR pathology lead for melanoma), A.E. (pathologist, RCPath representative), D.P.F. (pathologist, CAP representative), V.G.P. (pathologist, CAP representative), J.F.T. (surgical oncologist, RCPA representative), M.J.T. (pathologist, Canadian Association of Pathologists representative), M.Y.W. (pathologist, RCPath representative), and N.M.G.W. (pathologist, Canadian Association of Pathologists representative). The panel was directed to review the 3 existing protocols/data sets, use an evidence-based approach to harmonize them, and develop an organ-specific cancer data set based on ICCR's generic cancer data set.
The individual items in each cancer data set were classified as “required” (synonyms: core, mandatory, standard) or “recommended” (synonyms: noncore, nonmandatory, guideline). “Required” data elements were defined as those that have agreed evidentiary support at level III-2 level of evidence or above (Prognosis category, National Health and Medical Research Council [NHMRC])12 and that were unanimously agreed upon by the review panel to be essential for the clinical management, staging, or assessment of the prognosis of the cancer (later expanded to include key items fundamental for pathologic diagnosis). Required (core) items are mandatory and must be included in a pathology report on the specific cancer. Recommended (noncore) elements were defined as items of data that were unanimously agreed upon by the panel to be clinically important and recommended for good practice but for which the evidence for inclusion as requirements had not, to date, been supported by NHMRC level III-2 or above evidence.
Initially, the panel compared the existing structured pathology reporting protocols for cutaneous melanoma developed by the RCPA, RCPath, and CAP.7–9 Concordant pathology data elements were defined as those in which all 3 structured protocols both mandated the recording of a pathologic parameter as a core (required) element and had essentially similar methodologies for its assessment and reporting. Minor discordance was defined as inclusion as a mandatory element in 2 of the 3 national reporting systems or in which an element was included in all 3 but there were differences in its measurement or assessment. Major discordance was defined as inclusion of an item as mandatory in one national reporting protocol that was either included as a noncore item or not included in the other national protocols.
For the melanoma protocol, a project manager (M.J.J.) prepared an interactive questionnaire in conjunction with the chair for circulation to the panelists before their deliberations. This greatly simplified subsequent teleconference discussions and e-mail correspondence.
RESULTS
Comparison of the RCPA, RCPath, and CAP Pathology Reporting Protocols for Cutaneous Melanoma
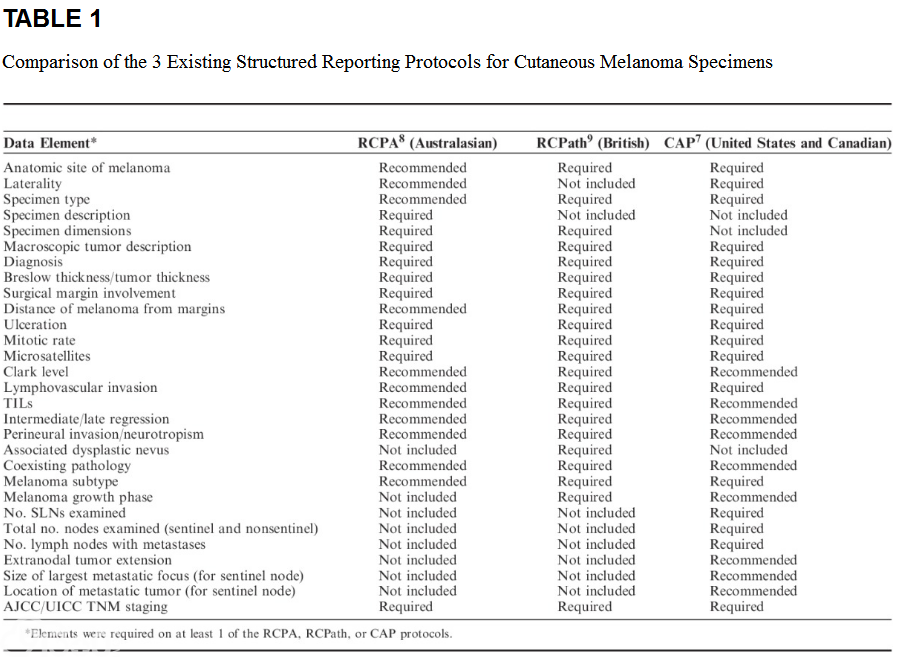
Multiple required/core pathologic parameters were collated from the 3 national structured reporting systems. In addition, the RCPA and RCPath reporting protocols mandate collection of clinical history and information on the surgical procedure. These additional parameters were not included in the comparison of protocols. Overall, as expected, there was good agreement between the 3 reporting systems (Table 1).
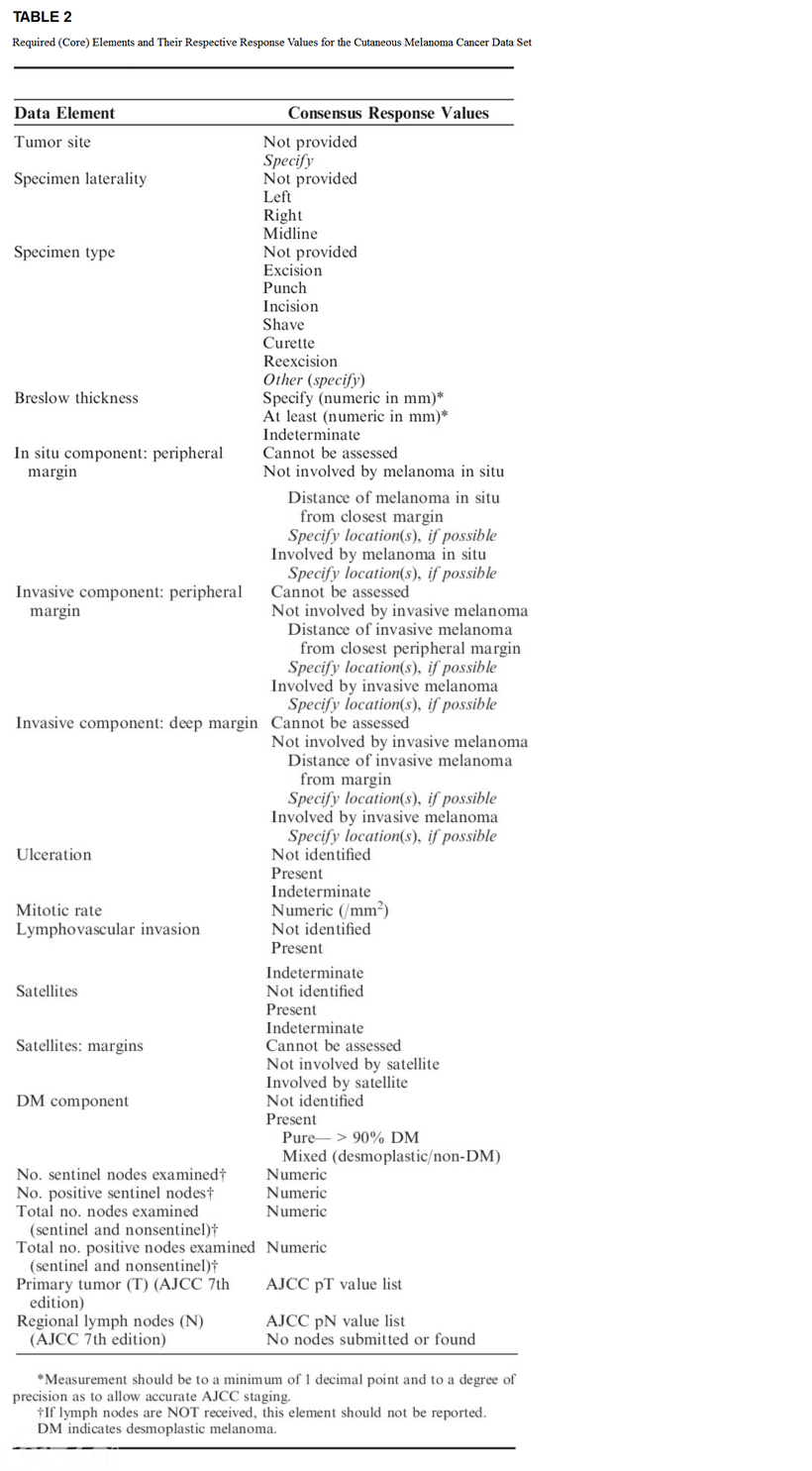
There were 8 concordant pathology data elements, and following the ICCR melanoma panel's review of the evidence base for each of these parameters, all were included as required (core) elements for tumor staging or prediction of prognosis (Table 2). There were another 6 pathologic parameters for which there was only minor discordance (Table 1). For instance, reporting lymphovascular invasion is mandatory in the CAP and RCPath reporting protocols, but it is only recommended as a best practice reporting guideline (recommended/noncore) in the RCPA protocol, reflecting differing weight given to the published studies. The review panel found that there was sufficient evidence—that is, at least NHMRC level III-2—to include 5 of these in the required (core) data set (Table 2). For example, while all protocols were in agreement that the presence or absence of surgical margin involvement was a mandatory reporting element, the RCPA protocol did not mandate reporting measurement of the distance of the melanoma from the margins. On reviewing the evidence, the panel unanimously agreed that this should be a required data element in the ICCR melanoma protocol. For the remaining minor discordant item (melanoma subtype), the panel considered that there was insufficient evidence to include it as a mandatory item, but it was still included in the recommended (noncore) list of items (Table 3).
There were a number of parameters that had major discordance between the protocols (in which they were included as a core item in only 1 of the protocols). After review of the evidence, some of these, as discussed in detail below, were included as ICCR core elements, some were included as noncore/recommended elements, and some were not included as either core or noncore items.
The RCPA and RCPath protocols did not include any data elements for the pathologic reporting of lymph nodes in conjunction with primary cutaneous melanoma (presumably because lymph node specimens are not routinely received at the time of a primary cutaneous melanoma biopsy). Because the status of the regional lymph nodes is a key staging parameter in the current version (seventh edition) of the American Joint Committee on Cancer Staging (AJCC) System for cutaneous melanoma,13–16 the review panel considered that, under the condition of receipt of lymph nodes in conjunction with a primary cutaneous melanoma, reporting of lymph nodes was a required reporting element. Further, it was recommended that if lymph nodes are NOT received, the data elements relating to lymph nodes should not be included in the pathology report (to avoid confusion, particularly in the minds of patients, who, upon reading the pathology report that states “Number of sentinel lymph nodes examined: zero,” may question why lymph nodes had not been removed).
Finally, there were reporting elements that were not included as mandatory reporting elements in any of the national protocols that the panel considered had sufficient evidence (ie, at least NHMRC level III-2) to warrant inclusion as core items. In some instances, this may have occurred because there was not sufficient evidence to justify inclusion when the protocols were developed. For example, the presence of a desmoplastic melanoma (DM) component was not included as a mandatory reporting element in any of the protocols. However, the panel considered that there was now sufficient evidence to include this as a core/required element.
The definitions, consensus response values (permitted responses) and key evidence for each of the required and recommended data elements are briefly summarized below.
REQUIRED (CORE) ELEMENTS
General Clinical Data Elements
Apart from the standard information required for patient and treating clinician identification, the melanoma cancer review panel identified a number of clinical elements as required (core) data elements in the cutaneous melanoma pathology report: tumor site, specimen laterality, and specimen type (Table 2).
Tumor Site
Accurately identifying the anatomic site of the primary melanoma is important for a number of reasons. Sufficient information is required to localize the lesion for subsequent therapy. A diagram or photograph can facilitate this.17,18 Further, when matched for other known prognostic factors, melanomas in the head and neck area, upper back, and axial skeleton have a worse prognosis than extremity-based lesions.19–21 The anatomic site of the tumor may also affect the pathologic interpretation of the histologic features observed, and this may, in turn, influence the proffered pathologic diagnosis. For example, nevi occurring on certain sites (including the palms, soles, fingers and toes, flexural sites, genitalia, the breast, and ear) often display features that would be considered evidence favoring melanoma in melanocytic tumors occurring at other sites.17,18,22–24
Specimen Laterality
Specimen laterality information is needed for identification purposes and to localize the lesion for subsequent therapy.
Specimen Type
Although clinical considerations are important in determining the most appropriate biopsy technique for a melanocytic tumor, the type of biopsy performed may affect the accuracy of pathologic evaluation.3,25,26 At times partial biopsies are performed of melanocytic lesions. Possible reasons include a very low suspicion of melanoma, the melanocytic lesion being large or located in a cosmetically sensitive area, and, in some instances, no clinical suspicion of the lesion being melanocytic (eg, many melanocytic lesions exhibit no clinical pigmentation). Further, correlation of the type of procedure with the material received can be important for patient safety. For instance, if the clinician states that the procedure was a punch biopsy but the specimen examined is a skin ellipse, it is possible that there may be a misidentification of the specimen.
An excision biopsy with narrow clearance margins is usually the most appropriate method of biopsy of a clinically suspicious melanocytic tumor. This enables an accurate assessment and will allow definitive treatment to be planned appropriately if a diagnosis of melanoma is confirmed.
Incomplete biopsies of melanocytic tumors (punch, incision, curette, and some superficial shave biopsies) may contribute to pathology misdiagnosis, because of unrepresentative sampling of a heterogenous tumor (ie, a partial biopsy may sample only the benign part of a lesion and miss a coexisting melanoma) or may not provide sufficient tissue for adequate assessment of the pathologic criteria necessary to permit correct diagnosis.26–28 Nevertheless, it remains an accepted clinical practice to partially sample melanocytic tumors in some instances, such as large pigmented lesions in surgically challenging locations—for example, the face or digits.
Pathologic diagnostic criteria for melanoma include features at the peripheral and deep aspects of the tumor, which may not be included in an incomplete biopsy. Another potential pitfall of an incomplete biopsy of a nevus is that it may regrow from residual nevocytes after incomplete removal. Regenerating nevi often display many histologic features that commonly occur in melanomas (including pagetoid epidermal invasion, cytologic atypia, occasional dermal mitotic figures, and HMB-45 positivity). For these reasons, such lesions have been termed “pseudomelanomas” and are prone to overdiagnosis as melanomas.29–31
Incomplete biopsies of melanomas may also provide inaccurate assessment of important pathologic features, such as Breslow thickness. Accurate assessment of pathologic features of a primary melanoma allows prognosis to be reliably estimated; it also guides selection of appropriate management (width of excision margins, appropriateness of sentinel node biopsy); inaccurate pathologic assessment can lead to inappropriate (usually insufficient) therapy.
Breslow Thickness
Breslow thickness is the single most important prognostic factor for clinically localized primary melanoma.19 Breslow thickness is measured from the top of the granular layer of the epidermis (or, if the surface is ulcerated, from the base of the ulcer) to the deepest invasive cell across the broad base of the tumor (dermal/subcutaneous) as described by Breslow.18,32,33 Deep, vertical extensions of the tumor, perpendicular to the base, should be assumed to be periadnexal and should not be included in the Breslow thickness (see also below).
To promote consistency in the evaluation of the Breslow thickness, the melanoma committee considered that the following points were worthy of note:
The Breslow thickness can only be evaluated accurately in sections cut perpendicular to the epidermal surface. Otherwise, a note should be included indicating that “the section is cut tangentially and an accurate Breslow thickness cannot be provided.” Nevertheless, in some tangentially cut sections, it is often still possible to report a tangentially measured tumor thickness. The latter may be clinically useful, because it can be reasonably inferred that the true Breslow thickness must be less than this measurement, and, when appropriate, this should be stated clearly in the report. At other times, particularly when the epidermis is not visualized, no tumor thickness can be provided, and supplementary prognostic information must be obtained from other factors (including ulceration, mitotic rate, and Clark level). When sections have been tangentially cut, it may be fruitful to melt the paraffin block and reembed the tissue as it may then be possible to obtain perpendicular sections for determination of the Breslow thickness.
The Breslow thickness should be measured in the standard way when there is dermal regression (ie, dermal regression extending to a greater thickness than the melanoma should not be included in the measurement of Breslow thickness).
In the case of periadnexal extension of melanoma (ie, in the adventitial or extra-adventitial tissue immediately adjacent to skin appendageal structures usually apparent as an extension or “tongue” of tumor extending beyond the depth of the main tumor mass), it is uncertain from current evidence where the measurement of tumor thickness should be made to most accurately predict patient prognosis. (This does not include adnexal involvement by melanoma, which is regarded as in situ disease.) The committee agreed that thickness measurements should not be based on periadnexal extension (either periadnexal adventitial or extra-adventitial extension), except when it is the only focus of invasion. In that circumstance, Breslow thickness may be measured from the inner layer of the outer root sheath epithelium or inner luminal surface of sweat glands, to the furthest extent of infiltration into the periadnexal dermis. The depth of extension of such foci beneath the granular layer of the epidermis may also be measured and reported (but it should be clearly stated how the measurements were obtained and that the periadnexal measurement represents the estimated “true” Breslow thickness).
The Breslow thickness cannot be determined if a superficial biopsy transects a melanoma and includes only its superficial portion. In such instances, the pathologist can only report the melanoma to be “at least” a certain thickness. Correlation with the reexcision specimen is necessary.
Other problems may arise from differing interpretations of the nature of dermal cells (ie, whether they represent melanoma or a preexisting nevus) and of tumors with verruciform architecture.
The inclusion of neurotropic spread of melanoma in the measurement of Breslow thickness is controversial. In this instance, it is recommended that the thicknesses of the tumor including and excluding the neurotropic component be recorded in the pathology report.
Satellites, as discussed in detail below, are foci of tumor discontinuous from the primary melanoma (probably representing local metastases) and should not be included in the measurement of tumor thickness.
In some instances, particularly when a melanoma arises in association with a nevus, it may be difficult to distinguish small “nevoid” melanoma cells from nevus cells, and this may have implications for measuring tumor thickness. Careful assessment of architectural and especially cytologic features should assist in distinction, but at times this remains difficult, subjective, and prone to interobserver variability.
The standard method for measurement of tumor thickness in ulcerated lesions may lead to an underestimate of thickness, because the recommended measurement from the base of the ulcer to the base of the tumor makes no allowance for the amount of tumor lost through ulceration.
The thickness (measured from the top of the granular layer) of any zone of regression may also be recorded in the pathology report (but it should be clearly stated that it does not represent the Breslow thickness).
Surgical Margin/Tissue Edges
The melanoma review committee considered that all cutaneous melanoma must document the relationship of both the in situ and invasive components of the melanoma to the nearest resection margins. For the invasive component, both the deep and peripheral margin must be recorded separately.
The pathology report should document the:
In situ component: peripheral margin.
Invasive component: deep margin.
Invasive component: peripheral margin.
The pathology report must indicate whether or not the invasive or in situ melanoma involves the surgical margins/tissue margins. If involved, the location(s) must be specified if possible. If not involved, the distance of the melanoma from the closest uninvolved margin must be recorded, and the location(s) of the closest uninvolved margins should be recorded, if possible. It was recommended that margin measurements to within the nearest 1 mm are sufficient for the purposes of directing further management. If the melanoma is within 2 mm of the resection line, it is34 recommended that the margin measurement be recorded to within the nearest 0.1 mm measurement.34
The standard treatment for primary melanoma is wide local excision of the skin and subcutaneous tissues around the melanoma. Such definitive treatment is not usually performed until after a pathologic diagnosis of melanoma has been established. The aim is complete surgical excision of all in situ and invasive melanoma components. Involvement of the surgical margin may result in regrowth or metastasis from residual melanoma and may adversely affect patient outcome.35–37 On the basis of several randomized controlled trials,38–42 national guidelines from several countries have recommended wide excision margins according to the thickness of the primary cutaneous melanoma.43–45 The trials were based on surgical margins measured clinically at the time of wide excision. Clinically measured wide excision margins are a less precise measure of the extent of excision of normal tissues surrounding the tumor than the histopathologic margins. However, there is very little evidence available for the relationship between histopathologic measured margin and local, in-transit, and regional recurrence.
Providing data on distance of melanoma from the margins may be helpful not only to clinicians in guiding patient management but also for pathologists when examining any subsequent specimen (eg, reexcision specimen or for determining whether recurrent tumor at the primary site represents local persistence of melanoma or a metastasis). Defining the peripheral extent of the epidermal component of a melanoma may be difficult and subjective particularly for melanomas arising in chronically sun-damaged skin in which the peripheral changes merge with those related to the effects of severe chronic sun damage and also for acral (and mucosal) melanomas.46
Ulceration
Ulceration is an integral component of the AJCC/UICC staging system and an independent predictor of outcome in patients with clinically localized primary cutaneous melanoma.33,47–49
Assessing the presence of ulceration may be difficult in recently biopsied lesions and in cases in which there is only a focal loss of the epidermis; in this case, it is difficult to determine whether the epidermal deficiency is due to ulceration or to sectioning artifact. Absence of fibrin or granulation tissue from putative areas of ulceration would be clues that the apparent ulceration is actually due to sectioning of only part of the epidermis.13
Mitotic Count
Multiple studies indicate that mitotic count is an important prognostic factor for localized primary melanomas (including very large studies utilizing the methodology for mitotic count determination described below).13–16,19,50–55
The number of mitotic figures can vary greatly between different parts of a tumor. For consistency and reproducibility, a standardized method must be used to assess mitotic count.56 It is recommended that the field diameter of a microscope be formally calibrated using a stage micrometer to determine the number of high-power fields that equates to 1 mm2.
In the seventh edition of the AJCC melanoma staging system, the recommended method to enumerate mitotic figures is to find an area in the dermis with obvious mitotic activity (the “hot spot”) and begin the count in this area, then extending the area counted to immediately adjacent nonoverlapping high-power fields in a 1 mm2 area. If no hot spot is identified and the mitotic figures are sparse and randomly scattered, then the count should begin in a field containing a mitosis, then extended to immediately adjacent nonoverlapping high-power fields until a 1 mm2 area of tissue containing melanoma is assessed. When the invasive component of the tumor involves an area <1 mm2, a 1 mm2 area of dermal tissue that includes the tumor should be assessed and recorded as a number/mm2. The number of mitotic figures should be listed as a whole number/mm2. If no mitotic figures are identified, the mitotic count may be recorded “none identified” or “0/mm2.” This methodology for determining the mitotic count of a melanoma has been shown to have excellent interobserver reproducibility including amongst pathologists with widely differing experience in the assessment of melanocytic tumors.13
It is also recommended in the seventh edition of the AJCC staging manual that the mitotic count should be assessed in all primary melanomas for prognostic purposes. However, it is only the presence or absence of mitotic figures in nonulcerated thin (≤1.0 mm thick) melanomas that impacts staging (ie, for separating pT1a and pT1b tumors).
The data that demonstrated the strong prognostic significance of mitotic count were obtained from the melanoma pathology reports of routinely assessed hematoxylin and eosin-stained sections. It is therefore not recommended that any additional sections be cut and examined (or immunochemical analysis be performed), in excess of those that would normally be used to report and diagnose the melanoma, to determine the mitotic count (ie, no additional sections should be cut and examined for the purpose of determining the mitotic rate; this includes the situation when no mitotic figures are identified on the initial, routinely examined sections).
Lymphovascular Invasion
Vascular invasion is identified by the demonstration of melanoma cells within the lumina of blood vessels or lymphatics or both. It is an uncommon finding in the excision specimens of primary cutaneous melanoma but is generally regarded as a marker of poor prognosis.57–60 There is a possible role for immunohistochemistry to highlight the presence of vascular invasion.57,61
Neurotropism
Neurotropism is identified by the presence of melanoma cells around nerve sheaths (perineural invasion) or within nerves (intraneural invasion).62–64 Occasionally, the tumor itself may form neuroid structures (termed “neural transformation”; this is also regarded as neurotropism).57,61,65 We recommend that pathologists be cautious not to overinterpret the presence of melanoma cells around nerves in the main tumor mass (which often represents “entrapment” of nerves in the expanding tumor) as neurotropism.
Infiltration along nerve sheaths (or occasionally within the endoneurium) may be associated with an increased local recurrence rate (local persistence).66 Neurotropism is common in DM (desmoplastic neurotropic melanoma) but may occur in other forms of melanoma.64,67–69 The presence of neurotropism is associated with increased risk of local recurrence and may, in some cases, be treated by wider excision margins and/or adjuvant radiotherapy.
Satellites
A microscopic satellite is any nest of metastatic tumor cells discontinuous from the primary tumor (but not separated only by fibrosis or inflammation). The terms “(micro)satellites,” “in-transit metastases,” and “local metastases” probably represent biologically identical processes with identical (worse) prognostic implications.70–73 (Micro)satellites and in-transit metastases are included in the same prognostic group by the AJCC.33,48,49,73
Satellites: Margins
The presence of a melanoma satellite metastasis at a peripheral excision margin may be an indication for reexcision, because it implies that there may be further melanoma in the skin beyond the visible margins.
DM Component
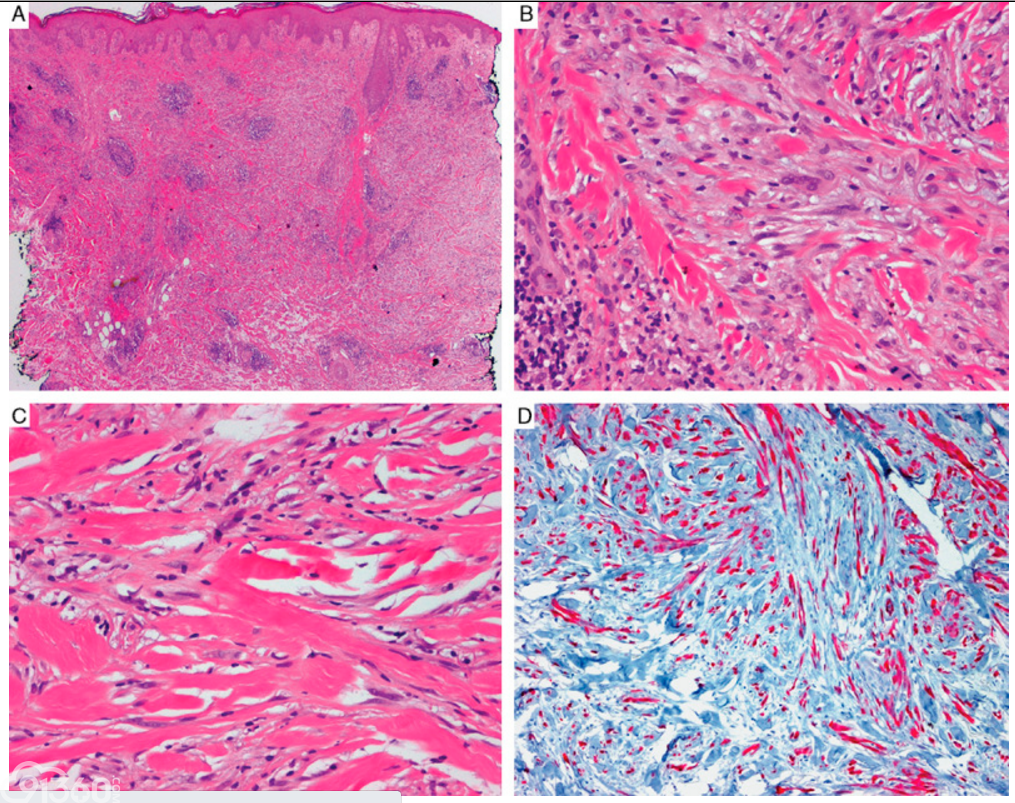
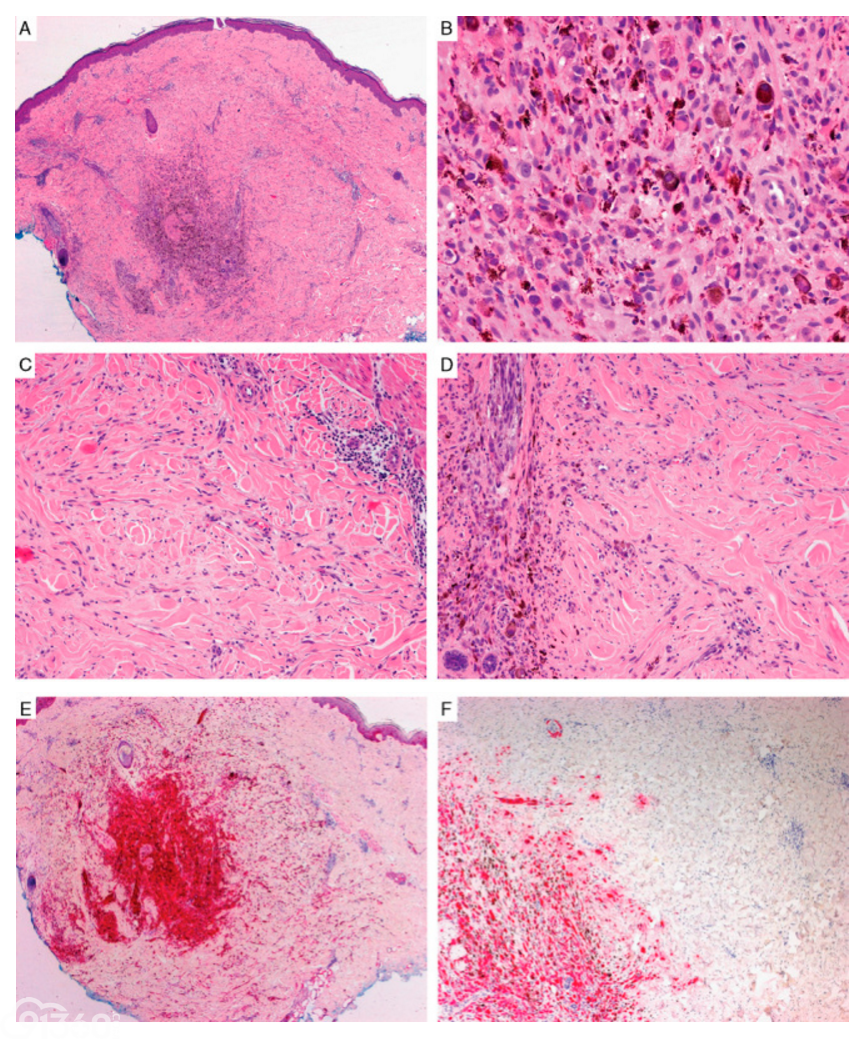
Desmoplastic melanoma is a rare subtype of melanoma characterized by malignant spindle cells separated by prominent fibrocollagenous or fibromyxoid stroma. Primary melanomas may be entirely or almost entirely desmoplastic (“pure” DM) (Fig. 1) or exhibit a desmoplastic component admixed with a nondesmoplastic component (“mixed” DM) (Fig. 2).74 In 2004, Busam and colleagues reported a clinicopathologic study of DM patients in which subdividing the tumors into “pure” and “mixed” subtypes correlated with clinical outcome.77 In that study, the authors classified melanomas as “pure” DM if “the overwhelming majority (≥90%) of invasive tumor was desmoplastic” or “mixed” DM if “typical features of DM were mixed with densely cellular tumor foci without fibrosis and desmoplasia” and the DM areas involved <90% and >10% of the invasive melanoma. Similar findings have since been reported by others.62–64,66,75–84 Improved disease-specific survival is seen in patients with “pure” DM, when compared with patients with “mixed” DM and those with melanomas lacking a desmoplastic component.62–64,66,75–84 Furthermore, regional nodal metastasis (including that detected by sentinel lymph node [SLN] biopsy) is less common in patients presenting with clinically localized pure DM compared with those who had mixed DM or conventional melanomas.62–64,66,75–84
FIGURE 1
DM, pure subtype. A–C, An atypical spindle cell proliferation involves the entire thickness of the dermis and is associated with desmoplastic/sclerotic fibrous stroma. Note the presence of scattered lymphoid aggregates. D, The spindle cells are positive for S-100 protein.
FIGURE 2
Mixed desmoplastic and non-DM. A–D, The tumor includes a heavily pigmented dermal “nodule” formed by large, variably pigmented, epithelioid cells that are surrounded by a more subtle proliferation of atypical spindle cells in a desmoplastic fibrocollagenous stroma. E, Both components are positive for S-100. F, The nondesmoplastic component is positive for HMB-45, whereas the desmoplastic component is negative for HMB-45.
Lymph Nodes
The committee considered that if lymph nodes are NOT received, this element should not be reported.
If lymph nodes are submitted, the following must be recorded:
The number of sentinel nodes examined,
The number of positive sentinel nodes,
The total number of nodes examined (sentinel and nonsentinel), and
The total number of positive nodes examined (sentinel and nonsentinel).
Any additional relevant microscopic comments should be recorded.
Tumor-harboring status of the SLN is the strongest predictor of outcome for clinically localized primary cutaneous melanoma patients.85–88
There are a number of potential pitfalls in the microscopic examination of SLNs.89 The most common diagnostic problem is distinguishing nodal nevus cells from a melanoma metastasis. This can usually be resolved by careful assessment of the location, morphologic features, and immunohistochemical staining characteristics of the cells and, in some instances, comparing the cytology of the nodal melanocytes with the cells of the primary invasive melanoma. Nodal nevi are usually located in the fibrous capsule and trabeculae of lymph nodes (but may rarely occur within the nodal parenchyma) and consist of small cytologically bland cells that are devoid of mitotic activity and, on immunohistochemistry, show strong diffuse positivity for S-100 and Melan-A, minimal staining for HMB-45, and a low (<2%) Ki-67 proliferative index. In contrast, melanoma deposits in SLNs are typically located in the subcapsular sinus or parenchyma and often comprise large, cytologically atypical cells with variably prominent nucleoli, mitotic activity, HMB-45 positivity, and Ki-67 positivity (variable but usually >2%).90,91 Other cells that may be found within lymph nodes and that are positive for S-100 include interdigitating (antigen-presenting dendritic) cells, nerves, and, occasionally, macrophages. These can usually be distinguished from melanoma cells on the basis of their location, size, shape, nuclear and cytoplasmic characteristics, distribution within the node, and immunohistochemical profile.92 Positive Melan-A/MART-1 staining of small numbers of cells in the intraparenchymal portion of lymph nodes from patients without a history of melanoma has been reported, and in our view caution should be exercised to not overinterpret isolated Melan-A/MART-1-positive (or HMB-45-positive) cells in SLNs as melanoma in the absence of other corroborative evidence (such as cytologic atypia, mitotic activity, or immunohistochemical positivity for HMB-45 and an increased high Ki-67/MIB-1 index). In our experience, the occurrence of such cells has become a more frequent diagnostic problem in recent years, presumably reflecting the utilization of more sensitive antibodies and immunohistochemical techniques.93,94 These cells could represent nevus cells, macrophages passively carrying melanoma-associated antigens, or some other cell type carrying antigens that cross-react with Melan-A/MART-1. Similarly, weak positive staining for HMB-45 is sometimes observed in pigment-laden macrophages.
AJCC Staging—Primary Tumor T Category (AJCC Seventh Edition)
In the seventh edition of the AJCC/UICC melanoma staging system, tumor thickness and ulceration continue to define T2, T3, and T4 categories. Moreover, T1b melanomas may also be defined by a dermal mitotic rate of ≥1/mm2 or ulceration, rather than Clark level of invasion (as in the sixth edition).49
Clark level IV or V is referred to by the AJCC as a tertiary criterion for T1b in cases with no ulceration and “if mitotic rate cannot be determined,”33 although we doubt that this scenario is likely to be encountered by pathologists in practice.
AJCC Staging—Regional Lymph Nodes N Category (AJCC Seventh Edition)
As per the AJCC staging recommendations, when insufficient information is available to determine the N staging subcategory at the time of reporting a primary melanoma, these should be recorded with an “x” (ie, Nx).
In the seventh edition AJCC/UICC Staging system, N1 and N2 categories remain for microscopic and macroscopic nodal disease, respectively (with SLN biopsy recommended for pathologic staging). Lymph node positivity is defined by the presence of melanoma cells identified on hematoxylin and eosin-stained sections or on sections stained by immunohistochemistry alone. Other criteria for the N category are satellites, in-transit metastases, and microsatellites. M staging continues to be determined both by the site of distant metastases and serum lactate dehydrogenase, but patients with regionally isolated metastasis from an unknown primary site should be categorized as stage III rather than stage IV, because their prognosis corresponds to that of stage III disease from a known primary site.
The AJCC staging committee eliminated the Mx designation from the seventh edition of the AJCC/UICC TNM system. Pathologic assignment of the presence of metastasis (pM1) requires a biopsy positive for cancer from a metastatic site.
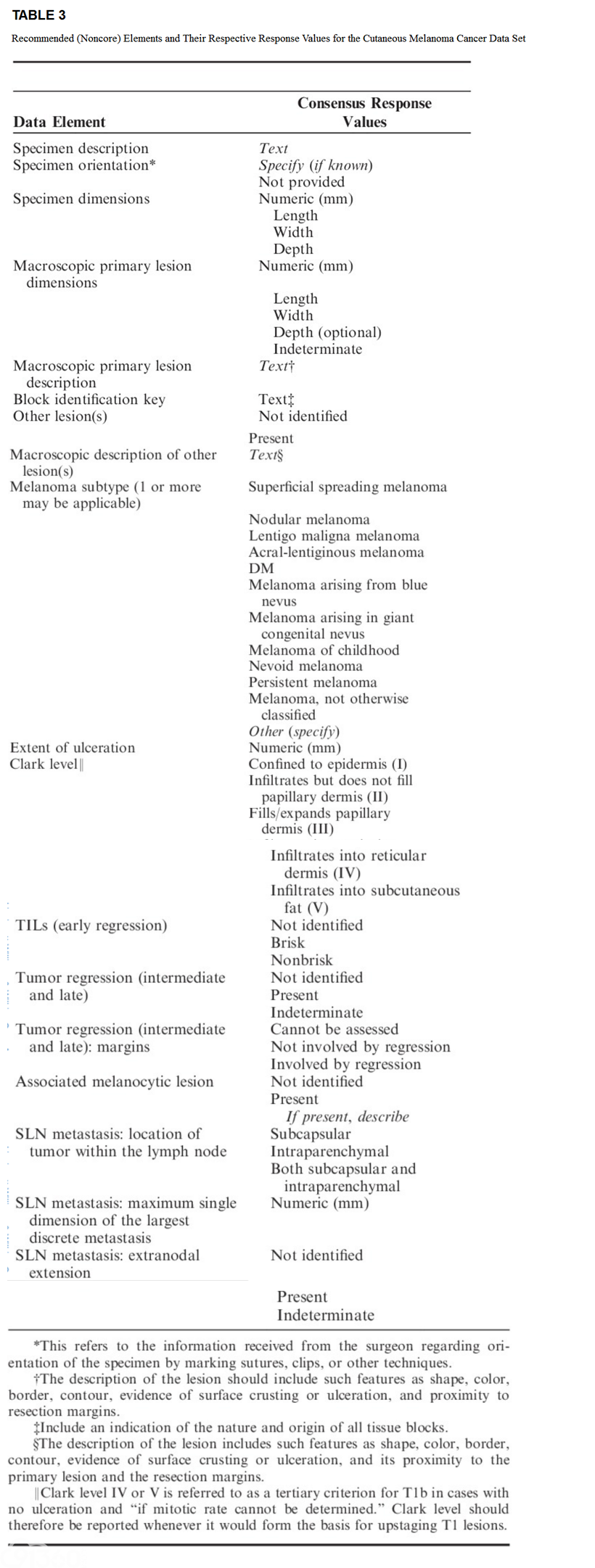
RECOMMENDED (NONCORE) ELEMENTS
Other Lesion(s)
Other lesions are often nevi or other benign lesions, but it is particularly important to identify the presence of satellite metastases because these portend a worse prognosis. (Table 3).
Melanoma Subtype
The common melanoma subtypes (superficial spreading melanoma, nodular melanoma, and lentigo maligna melanoma) have little, if any, prognostic significance independent of tumor thickness, interpretation is subjective and prone to interobserver variation,4,18,95–97 and their use is principally for clinicopathologic correlation. Nevertheless, the traditional (Clark) melanoma histogenetic classification highlights the myriad of clinical and histologic guises of melanoma, which if not recognized by clinicians and pathologists will potentially lead to a delay in diagnosis and a concomitant adverse clinical outcome.98 The traditional classification has been criticized because the criteria upon which it is based include clinical features (such as the site of the melanoma) and nontumorous histopathologic features (such as the character of the associated epidermis and the degree of solar elastosis) and also because of overlap in defining features, lack of an independent association with patient outcome, and minimal relevance as a determinant of clinical management.98
Epidemiological and molecular genetic evidence suggests that there are subgroups of melanoma that are associated with specific genetic alterations. The mutations indentified in melanomas have included NRAS (15% to 20%), BRAF (50%), KIT (2%), and GNAQ/GNA11 (50% of uveal melanomas). There are associations between the presence of some mutations and the anatomic site of a melanoma and the degree of solar elastosis.99,100 A comparison of the traditional clinicopathologic melanoma classification with a classification based on the somatic mutation status reveals remarkable similarities. For example, melanomas associated with prominent solar damage (lentigo maligna melanomas) commonly have NRAS and sometimes KIT mutations, whereas superficial spreading melanomas that arise in the skin of intermittently sun-exposed areas often have BRAF mutations. KIT-mutated melanomas most often involve acral (acral-lentiginous melanoma) and mucosal sites. Nevertheless, the degree of accuracy of the melanoma histogenetic subtype (or histopathologic assessment) for predicting the mutation status of a melanoma is not sufficient to replace mutation testing for the purposes of patient care.
Extent of Ulceration
Extent of ulceration (measured either as diameter or percentage of tumor width) provides more accurate prognostic information than the mere presence of ulceration.54,101–103
Clark Level
Clark level IV or V invasion is referred to as a tertiary criterion for T1b in cases with no ulceration and “if mitotic rate cannot be determined.” Clark level should therefore be reported whenever it would form the basis for upstaging T1 lesions. As discussed above, Clark level may also provide useful prognostic information if an accurate Breslow thickness cannot be determined.
Most evidence suggests that the Breslow thickness of a melanoma is a more accurate prognostic indicator than the Clark level.19 In the 2010, seventh edition of the AJCC melanoma staging system, Clark level is no longer used as a primary criterion for the definition of T1b tumors (which are now defined by the presence of a dermal mitotic rate of ≥1/mm2 or the presence of ulceration) except in the instance referred to above.21,33,104
Tumor-infiltrating Lymphocytes (Early Regression)
To be regarded as tumor-infiltrating lymphocytes (TILs), lymphocytes must infiltrate and disrupt tumor nests and/or directly oppose tumor cells. The assessment and grading of TILs remains subjective and prone to interobserver variation, although agreement may be improved by instruction. Reports on the prognostic effect of TILs vary, but most suggest that the presence of “brisk” or dense TILs is associated with a more favorable prognosis.54,105,106 A recent report suggested a strong association between TIL infiltrates and sentinel node status and survival when utilizing a novel grading system.85 Absent TILs predicted SLN positivity in a number of recent studies.85,107
Tumor Regression (Intermediate and Late)
A host immunologic response may be directed against melanoma cells and may result in elimination of part or all of the melanoma; this is termed regression. This phenomenon may be categorized into 3 temporal stages: early, intermediate, and late. Early regression is signified by the presence of TILs. Intermediate and late regression result in partial or complete loss of melanoma and are characterized by immature (intermediate) and mature (late) dermal fibrosis, often accompanied by the presence of melanophages and effacement of the rete architecture. Most reports assessing the prognostic significance of regression have not differentially analyzed intermediate and late regression.
The prognostic significance of (intermediate and late) regression is controversial.18 Some studies report that it portends a worse prognosis (particularly in thin melanomas),108 whereas others report that it is associated with a more favorable outcome.18 Difficulties in interpreting such studies include lack of a standardized definition or criteria for its diagnosis, selection bias, and poor interobserver reproducibility.
Tumor Regression (Intermediate and Late): Margins
Regression at a peripheral excision margin is an indication for reexcision, because it probably implies that there may be further melanoma in the skin beyond the visible margins.
Associated Melanocytic Lesion
Although of no known prognostic value, the recognition of an associated benign melanocytic lesion is relevant to the pathogenesis of melanoma and may be important for clinicopathologic correlation and epidemiological, clinical, and genetic studies.99 Documentation of an associated benign melanocytic tumor is also of relevance when there may be residual melanocytic tumor in the reexcision specimen and when knowledge of this may assist in the interpretation of the residual tumor overlying a scar as pseudomelanoma/recurrent nevus, rather than melanoma.
In some instances, it can be difficult or even impossible to determine whether part of the dermal component of a melanocytic tumor represents melanoma or an associated nevus. This is particularly the situation in melanoma composed of small, minimally atypical, “nevoid” cells or in cases in which the dermal component of a melanoma “matures” with depth.109 Careful assessment of cytologic characteristics—including the presence of mitotic figures and the identification of a second discrete cell population—may assist in some cases.
Sentinel Lymph Nodes
If the submitted SLNs contain metastatic melanoma, for each involved SLN, the pathology report should document:
the location of the tumor within the lymph node (subcapsular, intraparenchymal, or both),
the maximum single dimension of the largest discrete metastasis,
the presence or absence of extranodal extension.
Histologic parameters of melanoma deposits in SLNs have been shown to be predictive of the presence or absence of tumor in non-SLNs and clinical outcome.110–123 If there are only a small number of metastatic melanoma cells in the subcapsular sinus of the SLN, the patient's prognosis is very good and the chance of finding additional metastases in a completion lymph node dissection specimen is very small. However, if there are multiple large deposits of melanoma cells that extend deeply into the central part of an SLN, the prognosis is much worse, and the chance of finding additional metastases in non-SLNs in a completion lymph node dissection specimen is much higher. SLN parameters predictive of non-SLN status and survival include the size of metastases, tumor penetrative depth (also known as maximal subcapsular depth and centripetal thickness and defined as the maximum distance of melanoma cells from the nearest inner margin of the lymph node capsule), the location of tumor deposits in the SLN, the percentage cross-sectional area of the SLN that is involved, and the presence of extracapsular spread. However, the power of individual features of melanoma metastases in SLNs to predict tumor in non-SLNs, as well as survival, reported in some studies has not been reported by others. The determination of some of these parameters may not always be reliable, because tumor deposits are often irregularly shaped, the limits of tumor deposits can be difficult to discern, and tumor burden is to some degree dependent on sectioning protocols, as more extensive sectioning may reveal additional tumor deposits or demonstrate a greater dimension of deposit(s) in the deeper sections.124
DISCUSSION
The pathology report is critical in determining the management of patients with primary cutaneous melanoma. The information contained in the report not only influences management decisions, such as the width of excision margins, the need for skin grafts or other reconstructive procedures, the appropriateness of SLN biopsy, and participation in clinical trials but also has a major impact on predicting patients' prognosis. Melanoma patients with suboptimal pathology reports may be staged inadequately, managed poorly, and thus may ultimately experience an adverse clinical outcome. Clear communication between pathologists and clinicians is essential. The use of a structured report with predefined data elements and acceptable response values can facilitate this communication. It not only helps to ensure completeness of pathology reports but also consistency in reporting.3–6,18,125 In a structured format, the information is presented in a predictable and easy-to-read form. Further, the stipulation of acceptable predefined values can save time for the person completing and typing the report. In addition, a structured pathology report facilitates efficient extraction of information for registries, data collection, and research purposes.1–5 In studies assessing patients with breast carcinoma, colorectal carcinoma, and melanoma, it has been demonstrated that structured pathology reports are more complete and that clinicians find it easier to glean the clinically pertinent information from them.5,6,126,127
It should be emphasized that, although structured pathology reporting provides the framework for the minimum set of features to be assessed, it by no means restricts the pathologist to documenting only those features. All structured pathology reports must include the facility for free text comments. For melanocytic lesions that are difficult to classify as either a melanoma or a nevus and also for quality assurance purposes, the inclusion of a narrative element in a pathology report is useful, because it documents the histopathologic features used to justify a diagnosis and can provide a description of any difficulties encountered in assessing microscopic features. For melanocytic lesions that are difficult to classify, we recommend that the evidence in favor and against the particular diagnosis be presented and a preferred or favored diagnosis be provided, along with the degree of uncertainty.3,128,129 In cases in which there is genuine doubt about the correct diagnosis, it is usually appropriate to seek a further opinion from 1 or more experienced colleagues. If a malignant diagnosis is favored, the structured report template may also be completed. The template may be prefaced with comments such as “if melanoma the lesion would have the following features:.” Structured pathology report templates may need to be tailored to the requirements of the individual center. In doing so, it will be important that although additional items may be included according to local needs, the required and recommended elements listed above must retain the same naming conventions, units of measurement, value lists, and methods of assessment if valid comparisons are to be made throughout the world.
It is important to note that any pathology reporting protocol will require modification from time to time as new scientific data emerge. New prognostic markers in melanoma patients (such as tumor necrosis) are regularly reported and once validated in independent data sets may warrant inclusion in future versions of this protocol.130 Therefore, such protocols must be frequently reviewed and updated to be of maximal value. In recent years, with the development and refinement of new technologies (particularly various “-omics” platforms) and their exponentially reducing cost, there have been great advances in our understanding of tumor biology.131 As we move rapidly into an exciting new era of “personalized” medicine, it is hoped that new biomarkers will be identified to make it possible to tailor delivery of the most appropriate treatment at the optimal time.131 It will be important that, once validated, such biomarkers be incorporated into future iterations of cancer-reporting protocols. However, at present, there are no ancillary tests currently used on a routine diagnostic basis for primary cutaneous melanoma. For most melanomas, immunochemistry is not required to establish a pathologic diagnosis of melanoma. Nevertheless, in some instances it (eg, HMB-45 and Ki-67 labeling) may be helpful in determining whether a primary melanocytic tumor is benign or malignant.18 Recent studies using comparative genomic hybridization and florescence in situ hybridization have shown that these techniques can be utilized to distinguish melanomas (which usually harbor numerous chromosomal aberrations) from nevi (which rarely harbor any aberrations).132–138 One recent study suggested that florescence in situ hybridization may also provide prognostic information in melanoma patients, but this requires further validation.
With the recent development and testing of new promising targeted therapies for patients with metastatic melanoma,139–141 molecular pathology mutation testing for BRAF, NRAS, KIT, and other mutations has become common in many melanoma treatment centers. At the present time, routine mutation testing is recommended only in patients with inoperable AJCC stage III or stage IV disease (and will therefore usually not be performed at the time of diagnosis of primary cutaneous melanoma), and mutation testing was not included in the current version of the ICCR melanoma pathology reporting protocol.
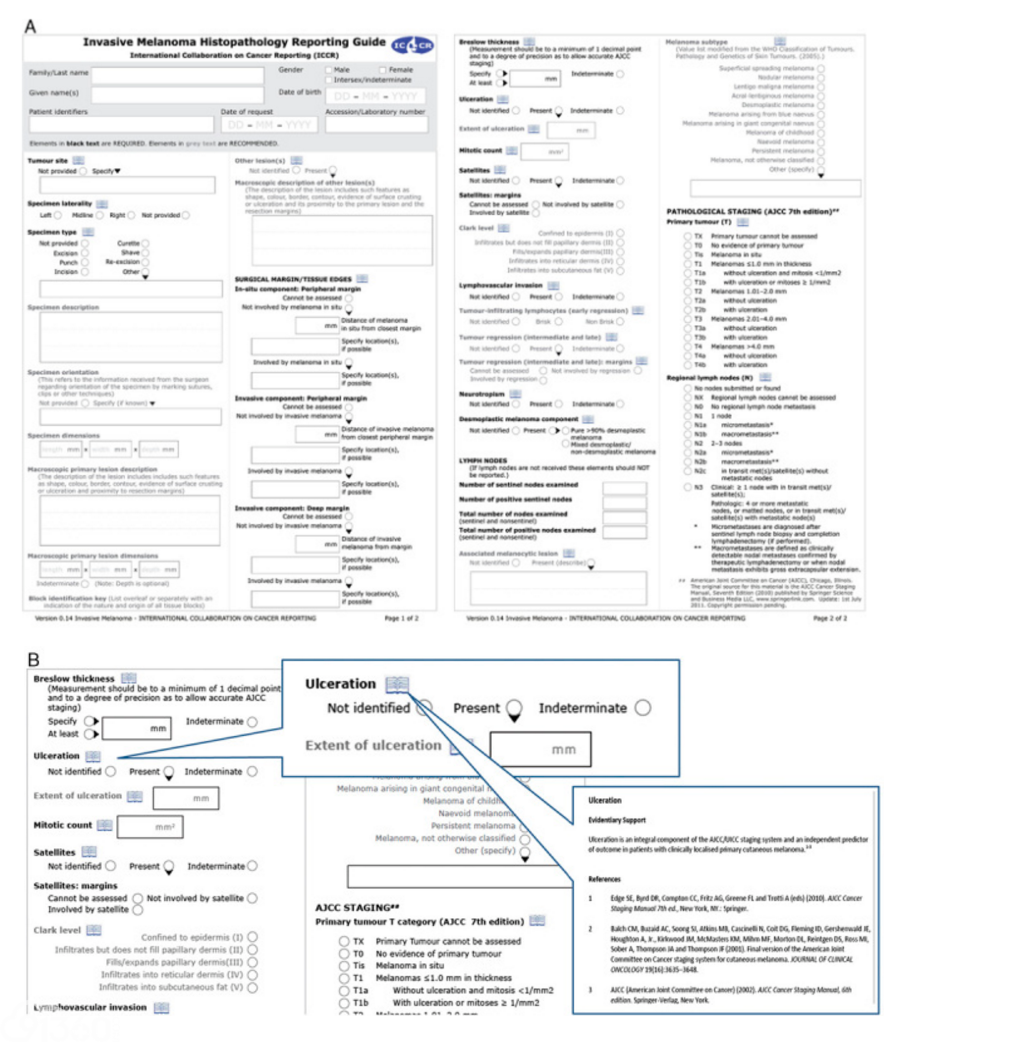
In conclusion, this manuscript describes the process and evidentiary review in the development of the ICCR cutaneous melanoma pathologic reporting protocol. The protocol, developed by an international committee of pathologists and clinicians with acknowledged subspecialty expertise, defines a list of 16 required/core data points that must be recorded in all cutaneous melanoma pathology reports (with an additional 4 required/core elements for specimens received with lymph nodes). In addition, to minimize ambiguity and to facilitate electronic implementation, the protocol specifies the list of response values for each of the data elements. There are also 18 recommended/noncore data points that should also be reported. This data set has been developed as part of the ICCR initiative, representing a quadripartite alliance between the Pathology Colleges of the United States, United Kingdom, Canada, and Australasia. It has subsequently been submitted for open international review with the aim of producing a globally agreed upon standard for the reporting of melanoma. After collation of all international responses, and review by the authors, the final data set will be published on the ICCR website (Fig. 3).142 An internationally agreed upon, structured pathology data set for melanoma is a prerequisite for research and for benchmarking in health care, while improving the consistency, completeness, and quality of melanoma pathology reports worldwide. The ICCR is currently engaged in working with a number of key international organizations to develop universally agreed upon standards for the pathology reporting of other cancers.
FIGURE 3
A, Invasive Melanoma Histopathology Reporting Guide. B, Invasive Melanoma Histopathology Reporting Guide excerpt.
【本站为非盈利学术交流平台,部分资料来源于网络,如涉及版权问题请及时联系管理员处理;所有文章仅供公益交流,不代表本站立场。欢迎提供素材、资料等,投稿邮箱:tougao@91360.com,一经采纳将给予稿费。】
| 





 发表于 2017-12-20 18:30:53
发表于 2017-12-20 18:30:53