登陆查看更多优秀资源帖,与同道便捷交流讨论
您需要 登录 才可以下载或查看,没有帐号?立即注册
x
SECTION1 第一部分
A 30-year-old woman presented with a history of generalized tonic-clonic seizures since childhood, occurring for the first time at age 9. The initial diagnostic workup at age 13 demonstrated a distinctive calcified mass of the left frontal lobe on CT (figure, A)。 Together with a single facial nevus, the lesion was suspected to represent Sturge-Weber-like phakomatosis; however, the patient's clinical history and physical examination failed to reveal further evidence of a neurocutaneous syndrome. Neither MRI nor biopsy for histologic confirmation of the diagnosis was performed. At age 18 the patient was lost to follow-up at the children's hospital.
30岁女性,自童年起有全身强直-痉挛发作病史,第一次发作时患者9岁,初次诊断是在13岁时,CT检查发现左侧额叶见明显钙化的肿块(图,A),加上面部有一处单发痣,该病灶被认为是Sturge-Weber样斑痣性错构瘤病。但患者的临床病史及体格检查均未发现神经皮肤综合征的进一步证据。未行MRI检查或旨在取得组织学确定诊断的活组织检查。18岁后患者从儿童医院失访。
At age 30, the patient, who had been on permanent antiepileptic treatment with valproic acid, had a generalized seizure, prompting clinical and radiologic reassessment. The reported facial nevus was no longer detectable and the patient was free of neurologic symptoms or signs. CT scan of the head revealed calcified masses of the left and right frontal lobes (figure, B), with considerable progression when compared to the initial CT scans obtained 17 years before.
患者虽然一直服用丙戊酸抗癫痫治疗,但30岁时一次全身发作敦促临床及放射学重新评估。前述面部痣已消失,患者无神经系统症状或体征。头颅CT扫描显示双侧额叶钙化性肿块(图,B),比17年前初次CT扫描时明显进展。
SECTION2 第二部分
In the absence of significant clinical findings, the radiologic differential diagnosis based on CT scans is broad, including various primary and secondary brain tumors. Neoplasms with dense calcifications include, among others, oligodendroglioma, ganglioglioma, and meningioma. Vascular pathologies including cavernous malformations or aneurysms and infectious lesions with calcifications such as tuberculosis must be considered. Furthermore, Sturge-Weber syndrome and other neurocutaneous disorders can be associated with cortical calcifications. More advanced imaging techniques may be helpful to allow for a more precise diagnosis. An MRI scan confirmed the bifrontal masses with distinctive signal alterations on T1- and T2/fluid-attenuated inversion recovery (FLAIR)–weighted sequences of the surrounding brain parenchyma interpreted as chronic demyelinating and gliotic changes rather than acute vasogenic edema, consistent with the slow progression of the lesion.Contrast-enhancedT1sequences demonstrated intense contrast enhancement in the noncalcified regions of the lesion (figure, C)。In order to assess the nature of the mass more precisely, 18F-fluoro-ethyl-tyrosine PET (18F-FET-PET) was performed, which displayed marked enhancement of tyrosine uptake compatible with metabolically active tissue (figure, D)。
没有重要临床表现的前提下,基于CT扫描的放射学鉴别诊断是比较广泛的,包括各种原发及继发性脑肿瘤,包括:伴致密钙化的肿瘤有少突胶质细胞瘤、节细胞胶质瘤和脑膜瘤等。血管病变包括:海绵状血管畸形或动脉瘤、伴钙化的感染性病变如结核都要考虑到。而且,Sturge-Weber综合征及其它神经皮肤病变可合并皮层钙化。进一步影像学检查有助于提供更为准确的诊断。MRI扫描显示在T1、T2及FLAIR序列周围脑实质慢性脱髓鞘及胶质增生而非急性血管源性水肿(提示病变进展缓慢)的背景下,双侧额叶肿块有明显信号改变。对比剂增强T1序列显示病变非钙化部分明显强化(图,C)。为更准确评估肿块特性,进行了18F氟乙基酪氨酸PET检查(18F-FET-PET),结果显示酪氨酸摄取明显增高,支持有代谢活性组织。(图,D)。
SECTION3 第三部分
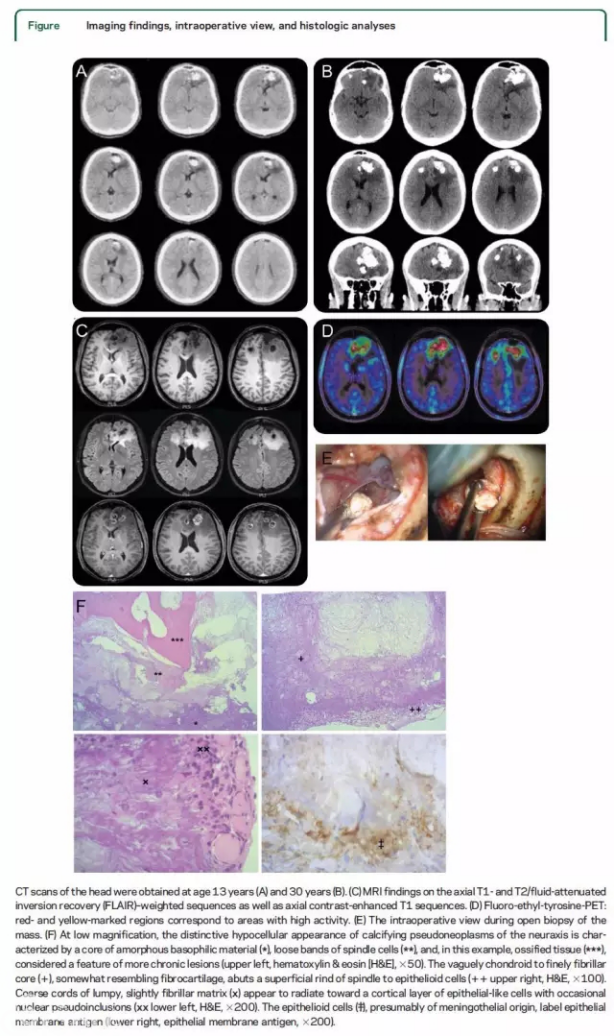
Overall,the imaging findings cannot be considered as typical of Sturge-Weber syndrome or any other neurocutaneous syndrome. However, the strong tyrosine uptake indicates metabolically active tissue and is suspicious for a malignant tumor. Based on these considerations, the decision was made to obtain a biopsy for histopathologic assessment. A microsurgical open biopsy was undertaken with neuronavigation guidance in a superficial isolated lesion including meningeal and cortical samples within high FET uptake and contrast enhancement (figure, E)。 On gross examination, the tissue was noted to have a gritty texture and contained white flecks. Histologic analysis revealed an unstructured hypocellular mass with an amorphous vaguely chondroid to finely fibrillar core, somewhat resembling fibrocartilage, surrounded by mature lamellar bone and a superficial rind of spindle to epithelioid cells (figure, F, upper panels)。 Coarse cords of lumpy, slightly fibrillar matrix appeared to radiate toward the cortical layer of epithelial-like cells. These plump cortical cells with nuclear pseudoinclusions (figure, F, lower left) were variably positive for epithelial membrane antigen compatible with meningothelial origin (figure, F, lower right)。 The MIB1 proliferation was low (,1%) and mostly restricted to the surfacecells. Based on the above features and the absence of other elements suggesting aneoplastic process, the diagnosis of “calcifying pseudoneoplasm of the neuraxis” was rendered.
总体而言,这些影像学表现不支持典型的Sturge-Weber或其它神经皮肤综合征。而且,明显的酪氨酸摄取提示代谢活性组织,需要考虑恶性肿瘤。基于这些考虑,最后决定行活组织检查进行组织病理学评估。在神经导航下对一处部位表浅病灶行显微外科切开活组织检查,将FET高摄取、对比强化区连同脑膜、皮层一起取样(figure,E)。大体病理显示,病变组织呈砂砾状,内见白色斑点。组织学分析提示为无结构、乏细胞肿块,有模糊软骨样-纤细纤维样无定形核心,有点类似纤维软骨,周围包绕成熟板层骨及梭形-上皮样细胞形成的包膜(图,F,上),粗大的团块状索条、细长的纤维基质向皮层侧上皮样细胞层放射状排列,这些含细胞核假包涵体(图F,左下)的肥大皮层细胞表达不同的脑膜上皮来源的上皮细胞膜抗原(图,F,右下)。增值指数MIB1低(,1%),多限于表面细胞。基于上述特点,且缺乏提示肿瘤病变的其它成分,诊断为“神经中轴钙化性假瘤”。
DISCUSSION 讨论
Calcifying pseudoneoplasms of the neuraxis (CAPNONs) are rare lesions of the CNS, with few patients reported to date.1–10 CAPNON can occur bothintracranially and spinally without a predominant localization. It has been described in patients aged from 6 to 68 years with a preponderance of males.3 The clinical symptoms and signs vary and dependon the localization of the mass, with seizures as the most frequent symptom if the lesion is located intracranially.1,2 Of note, CAPNON is a descriptive diagnosis and the underlying pathologic process is largely unknown. By definition, CAPNON is a discrete hypocellular, chondrocalcific, occasionally ossified mass that is covered by a surface layer of epithelioid cells of presumed meningothelial origin. According to the current interpretation, a reactive rather than a hamartomatous lesion has been assumed.2 Other authors have suggested that the lesion represents abortiveboneformation7 or an extremely rare variant of a very low-grade neoplasm.8 CAPNONs present with distinctive imaging features, as is illustrated in our case. CT scans typically show a densely calcified lesion,1 whereas MRI mostly reveals hypointense T1 and T2 signals with mild and inhomogeneous internal or rim contrast enhancement.1,4
神经中轴钙化性假瘤(CAPNONs)是罕见的中枢神经系统病变,目前仅有极少数报道。[1–10]CAPNON可发生于颅内及椎管内,没有确切好发部位,发病年龄从6岁到68岁均有报道,男性多见。[3]临床症状及体征因肿块部位而异,颅内病变以癫痫最常见。[1–2]值得注意的是,CAPNON是一个描述性诊断,基础病理过程大都不明确。从定义上看,CAPNON是一种异质性乏细胞、软骨钙化、偶见骨化的肿块,表面覆盖着由可能为脑膜上皮起源的上皮样细胞层。按照目前的解释,认为CAPNON是一种反应性病变,而非一种错构瘤样病变。[2]还有学者认为这种病变是骨的形成不全或极低级别肿瘤的罕见变异。[8]如我们这例所见,CAPNONs有明确的影像学特征,CT扫描常显示为致密钙化的病变,[1]而MRI多表现为T1、T2低信号,伴病灶内部或边缘轻度不均匀对比增强。[1,4]
The present case adds some novel aspects and is of particular interest because of the radiologic documentation covering a period of 17 years, which demonstrates that these lesions can grow over a very long period of time. Furthermore, this is the first report on the use of FET-PET in a patient with CAPNON. The MRI demonstrated marked contrast enhancement in the noncalcified peripheral regions of the mass and a distinct T2/FLAIR signal alteration (figure, C), which differs from other reports. Furthermore, our patient underwent an 18F-FET-PET scan, which displayed profoundly increased tyrosine uptake (figure, D); however, FET-PET has not been previously reported in patients with CAPNON. Of interest, the PET results suggest the presence of tissue with high activity. Together with the CT and MRI findings, this led to the initial assumption of a malignant tumor. However, the histopathologic features shown in our case did not support the diagnosis of a malignant tumor but displayed the characteristic features of CAPNON. The histopathologic differential diagnosis encompasses tumoral calcinosis as seen in neoplasms such as osteosarcoma, chondrosarcoma, meningioma, or even gliomas; however, histologic evidence of a neoplastic process was lacking. Alternatively, since the lesion could not be completely excised, another entity not sampled by the surgical procedure cannot be excluded.
这个病例跨度17年的影像学资料,显示这类病变在长期病程中缓慢增长,因此为该病补充了一些新的内容,值得关注。此外,这是首次FET-PET在CAPNON患者检查中应用的报道。MRI显示肿块非钙化的边缘区域显著对比增强及明显的T2/FLAIR信号改变(图,C)也与此前报道不一致,而且我们这例患者进行了18F-FET-PET扫描,也显示明显酪氨酸摄取增高(图,D),之前一直没有FET-PET在CAPNON患者检查中应用的报道。有趣的是,PET结果提示存在高代谢活性组织,结合CT及MRI表现,导致了初始诊断为恶性肿瘤。但组织病理学特点不支持恶性肿瘤,而表现为典型CAPNON的特点。组织病理学鉴别诊断包括肿瘤性钙质沉着症,诸如骨肉瘤、软骨肉瘤、脑膜瘤,甚至胶质瘤;但缺乏肿瘤性病变的组织学证据。当然,由于病变不能完全切除,不除外手术取材时遗漏其他性质的病变。
Our patient had a long-standing history of seizures that spanned more than 20 years. The radiologic documentation covers 17 years and indicates a clear progression of the lesion within this period. Resection has been proposed as the most appropriate treatment for CAPNON.3 However, large lesions as in our case may not be amenable to complete resection. Owing to the lack of larger series, the value of complete vs partial resection remains speculative. However, given the continuous growth of the mass in our patient, complete resection—if considered feasible without causing neurologic deficits—may be the preferred approach. Partial resection may help to reduce the mass effect and neurologic symptoms but may not prevent further growth. Because of the lack of any therapeutic approach other than surgery, complete resection may be the only option to prevent continuous growth of CAPNON as in our case. Another important aspect of surgery is the collection of tissue, which allows for histopathologic confirmation of CAPNON and the exclusion of other differential diagnoses.
我们这例患者有长达20余年的长期癫痫病史,17年的影像学检查资料提示病变在这段时间有确切进展。手术切除是CAPNON的最恰当的治疗方法。[3]但像我们这例中大而多发的病变可能无法完全切除。由于没有大宗病例证实,完全切除较部分切除的优势也只是推测。不过,鉴于我们这例患者肿块在持续生长,如果能在不引起神经功能障碍的前提下完全切除,这可能是首选方法。部分切除有助于减轻占位效应及神经症状,但不能阻止病变进一步生长。如我们这例所见,由于除了外科手术外没有其它治疗方法,完全切除可能是阻止CAPNON继续生长的唯一方法。手术的另一个重要作用是获取组织,从而进行CAPNON的病理学诊断,排除其它鉴别诊断。
The progressive growth pattern of the lesion in our patient and the high activity assessed by FET-PET challenge the view that CAPNON represents an entirely benign lesion, despite the lack of histologic signs of malignancy. Other treatment modalities in patients with nonresectable CAPNON have not been established so far and the potential benefit of medical treatment such as steroid administration or more aggressive approaches such as chemotherapy or irradiation needs further investigation.
除缺乏恶性病变组织学证据外,我们这例患者病变进行性生长的方式、FET-PET的高代谢活性都是对CAPNON为完全良性病变观点的挑战。不能切除的CAPNON患者的其它治疗方法目前尚无定论,激素等药物治疗或更为激进的放化疗的潜在收益有待进一步研究。
图:13岁(A)、30岁时(B)的颅脑CT。(C)MRI轴位T1-、T2/FLAIR及轴位对比剂增强T1序列。(D)氟乙基酪氨酸-PET:红、黄色标记区代表高代谢活性区。(E)肿块切开活组织检查的术中所见。(F)低倍镜下,神经中轴钙化性假瘤呈明显乏细胞表现:无定型嗜碱性物质核心(*),稀疏的梭形细胞带(**)及该例中所见的骨化组织(***),这些特点提示更为慢性的病变(左上,苏木精-伊红染色[H&E],×50)。梭形-上皮样细胞的包膜下可见类似纤维软骨的模糊软骨样-纤细纤维样核心( 右上,H&E,×100)。粗大索条状团块、纤细的纤维基质向上皮细样细胞的皮质层放射状排列(x),偶见细胞核假包涵体(xx左下,H&E,×200)。上皮样细胞(?)可能为脑膜上皮起源,可被上皮细胞膜抗原标记。(右下,上皮细胞膜抗原,×200)。
【本站为非盈利学术交流平台,部分资料来源于网络,如涉及版权问题请及时联系管理员处理;所有文章仅供公益交流,不代表本站立场。欢迎提供素材、资料等,投稿邮箱:tougao@91360.com,一经采纳将给予稿费。】
| 




 发表于 2017-12-20 18:30:54
发表于 2017-12-20 18:30:54